“Maternity Service Liaison Committees (MSLCs) provide a means of ensuring the needs of women and professionals are listened to and we saw how effective they could be when properly supported and led.”
“I urge you to play your part in creating the maternity services you want for your family and your community. Voice your opinions, just as you have during this review, and challenge those providing the services to meet your expectations.” (Julia Cumberlege, Chair of the Review Team, 2016)
These quotes really illustrate why MSLCs matter. They sum up why I am so passionate about maintaining and sustaining our wonderful Maternity Services Liaison Committee and helping others maintain theirs.
Because I have seen the difference a dynamic, properly supported, MSLC can make to a hospital Trust. Bromley MSLC, like its counterparts throughout the country, is a mix of individuals including commissioners, service users, midwives, doctors and other professionals coming together to monitor and improve local maternity services. The respect that everyone has for each other is evident in our meetings and some of the lightbulb ideas that arise are extraordinarily exciting. I tend to come away from meetings with my head reeling, but also tremendously grateful that we have this group of extraordinary passionate, dedicated people working and living in our area.
MSLCs were first established in 1984, enabling women to be involved in shaping the maternity care provided for them. The Department of Health suggests there should be an MSLC for each Trust in England and Wales. The Health and Social Care Act of 2012 states that health services at every level need to actively engage with service users:
Participating in planning and making decisions about their care
Enabling effective participation of the public in the commissioning process itself
So that services reflect the needs of local people.
Recommendation 13 from the 2015 Kirkup report into the Morecombe Bay Investigation also highlighted the importance of MSLCs.
MSLCs matter because…..
They are the only multi-disciplinary committee of its kind in maternity, bringing together commissioners, NHS Trust staff AND the women for whom the service is designed. One third of the committee is made up of service users, including a service user rep chair and vice chair.
They are independent NHS working groups that advise on commissioning and service development
They should include service users from all parts of the community, ensuring that all women’s voices are heard.
They promote collaboration and involvement
They plan, oversee and monitor maternity services in a local area and make recommendations for improvements where necessary.
They are one of the few examples in maternity where there is true collaboration between healthcare professionals and service users on equal terms at a local level. This leads to a much greater understanding between both parties of the challenges that are faced and the issues that really matter to local women.
The National Maternity Review also highlights the consensus among health professionals to change things for the better. Nowhere is this more evident than on an MSLC!
MSLCs can achieve amazing things:
They plan…..together with the commissioners, service users have the unique opportunity to help shape the future of the maternity services in the local area. For example, because of user testimonials provided by our MSLC to the clinical executive, a new perinatal mental pathway is being developed in our local area by the CCG, which will greatly benefit thousands of women.
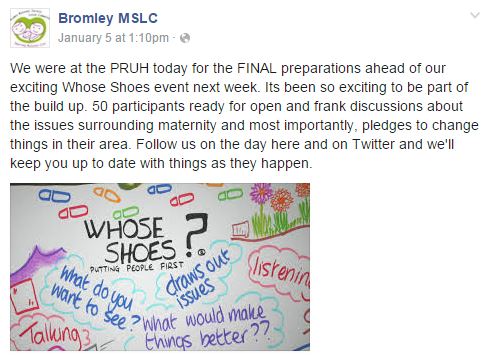
They oversee……our MSLC is involved in one off projects designed to improve maternity experiences for local women. We have designed information posters, are having an input into a “Welcome to the Ward” postnatal pack and have helped improve the birth environment on the Labour Ward. We also make tours of the wards, bringing a service user perspective and a fresh pair of eyes to the environment.
They monitor……our MSLC gains feedback from women through surveys, questionnaires and Walk the Patch both in the hospital and more recently in children centre health clinics in the community. That feedback is given directly to the lead health professionals of the Trust as well as the commissioners, who listen and act on our recommendations. Those improvements are then fed back to the service users, via social media and other means, so that we close the loop.
This type of work is not just being done by our MSLC. I know of countless other committees which are tirelessly working to improve services in their local area too. Our brilliant vice chair Michelle Quashie is planning a Women’s Voices conference in October and has asked me to present the achievements of our MSLC and others around the country, demonstrating how effective collaborative working can be. I am looking forward to showcasing just what has been and can be achieved then.
At our recent Whose Shoes event pledges were made at the end of the workshop about something that the delegates would do differently as a result of that day. These pledges have formed the workplan for our MSLC for 2016 and we will check to ensure that they have been carried out. MSLCs are true examples of #MatExp in action at a local level.
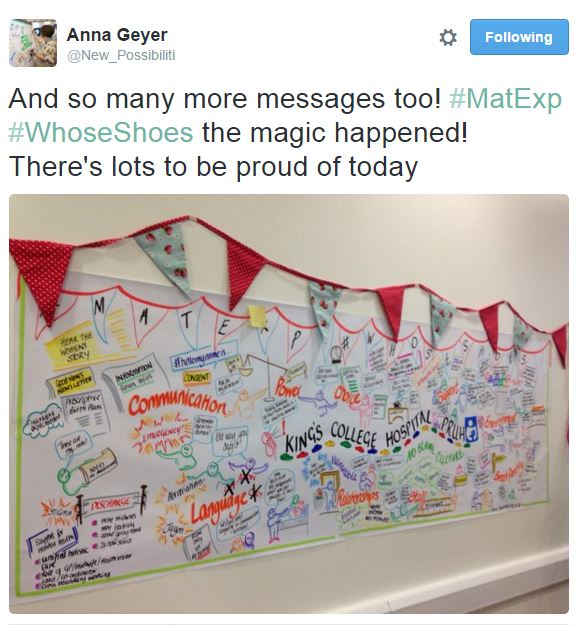
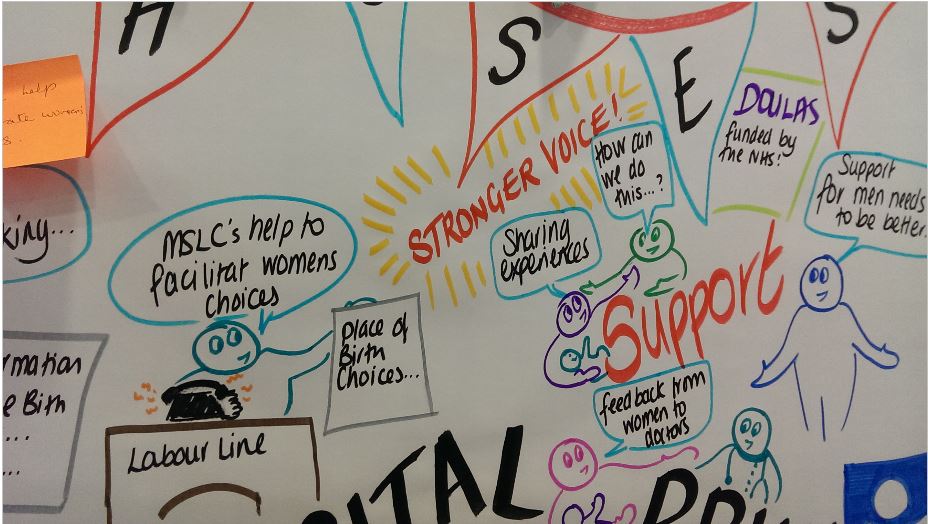
We were also really pleased to see the importance of MSLCs highlighted on our beautiful graphic courtesy of New Possibilities.
For this blog I asked members of other MSLCs for their thoughts on why MSLCs matter. Responses included:
“MSLCs matter because it is gives all that are passionate about a Women’s Maternity experience a chance to join forces and make their hopes for better birthing world a reality. It enables all members to be involved in ensuring this happens. It allows true collaborative working and keeps service users involved in decisions made about women’s maternity care and that of their family. It’s a safe place where women’s voices are heard, valued and respected. A Women’s experience is its driving force for that reason I am proud to be part of such a dynamic committee.
Initiatives like ‘Walk the Patch’ enable all women’s voices to be heard regarding the maternity care they are receiving. These voices from the community can then be filtered back to senior levels and actions are derived to improve the service as a result. WTP also gives the chance for those HCP that are providing truly women entered care the recognition they deserve.
I joined the MSLC after feeling very let down buy my personal maternity care. I knew I had to help change things for other women. Being part of the MSLC has enabled me to do that from the inside out. The work we have done and the wonderful HPs I have worked with has helped to restore my faith and feel empowered by being part of making change happen for others.
I hope that MSLCs get the recognition and support for the amazing work we are doing across the country. All that give up their time, do so because they are passionate and dedicated. MSLC’s should be mediatory for all trusts. How else can you ensure a woman centred service is given without women voices being heard in order to influence that service?”
Refreshed guidelines from NHS England, due for imminent publication, call for MSLCs to be run, maintained and funded by the CCGs. This is much needed, because in the current economic climate many MSLCs are fighting for modest but essential funding to continue the collaborative work they are doing. In addition, due to the unique nature of these committees it can be difficult for the commissioners to work out a mechanism for funding.
It is against this background, while MSLCs are struggling, that Julia Cumberlege, chair of the National Maternity Review, urges women in her introduction, “play your part…for your family and community … voice your opinions” as quoted at the top of this blog. MSLCs provide an ideal forum for service users to do just that. They are the ‘best practice model’ for shaping the future of our maternity services.
A petition has been started to emphasise the need for MSLCs in all areas. Please consider signing and sharing this petition so that MSLCs can continue the vital collaborative work they are doing at a local level, with volunteers’ expenses paid and commissioners everywhere listening and learning. https://petition.parliament.uk/petitions/121772
If you are not already involved with a local maternity group that feeds into an MSLC – or the MSLC itself, search online to see what you can find out about local provision. Contact your local CCG, your head of midwifery, local Healthwatch, or any pregnancy and parenting groups, such as the NCT and find out what’s happening. You can find out more about MSLCs at https://www.nct.org.uk/professional/mslcs
Some really exciting developments with #MatExp Whose Shoes? at the moment.
Bromley MSLC produced a ‘one year on’ report following up on their Whose Shoes? workshop at King’s College hospital using “I said, I did” as a framework to list all the fantastic outcomes that had come from pledges made on the day.
Language continues to be a big issue for women and families, but some great initiatives are now happening. Building on the Whose Shoes? workshops, Leeds and Colchester in particular are working on specific language challenges. I came up with a ‘Negativity Bingo’ and had great fun with my team at the NHS Fab Change Day #DoAthOn event launching #DumptheDaftWords.
I have been getting some exciting invitations to speak about building social movements and of course gave #MatExp a big shout out in my talk at the launch of #AHPsIntoAction, they have invited me back for a longer keynote session at their annual conference in June.
More hospitals are coming on board with the Whose Shoes? approach – the energy is particularly strong in London, the West Midlands and the South West regions. It has been great to present on several occasions now with Catherine MacLennan and Emma Jane Sasaru and to see people learning so much from their courageous sharing of their lived experience.
This slideshow requires JavaScript.
Last Friday, 3 Feb 2017, we were invited to present a #MatExp Whose Shoes? session to get some good discussions going as part of a packed event launching #PanStaffsMTP in Stafford. We concentrated specifically on continuity and perinatal mental health. This is the county-wide transformation programme to improve maternity experience in Staffordshire to implement the national ‘Better Births’ vision. This informal film gives you a flavour.
We are proud of the crowdsourced ‘Nobody’s Patient’ project and thank everyone for your fantastic contributions. We now have over 120 new Whose Shoes? scenarios and poems and the new resources will be made available shortly to all the hospitals who were existing customers. Florence Wilcock, Sam Frewin and I are finalising the supporting toolkit and collating the case studies, ahead of our ‘wrap up’ event in March. We are trying to pull together lots of ideas for positive change, with or without a workshop. I hope you are enjoying the regular Steller stories, including Florence’s monthly reports.
Wonderful to see everyone doing such amazing work, speaking all over the place, building networks, spreading the word and generally making great things happen.
Remember #Flaming June? This time last year we asked you to wake up, light the fires and take action to improve maternity experience. We gave you a template and asked you to share your action selfies with us. There were many resulting actions spilling out in all directions & across many geographical areas, some big and some small, some simple and completed, some complex and ongoing. Major highs were the birth of this wonderful MatExp.org.uk website and founding of the MatExp Facebook group. This June will I’m sure be no less exciting. From my own perspective I am taking a #MatExp poster to the RCOG world congress, we are hosting a stand & speaking at the London labour ward leads meeting, and of course we are in the middle of our new project ‘Nobody’s patient’ MatExp 2. I know there are two #MatExp Whose Shoes? workshops planned in June: Homerton & Colchester, the latest Trusts to jump on board, following fast in the footsteps of Cumbria last week. #MatExp certainly never stops moving and I know many of you are busy at work on numerous actions in all sorts of directions. Fabulous stuff!
I have written a few reflective blogs in the past to look back and take stock of what we have achieved since #MatExp started in October 2014, but for a change this time to mark the anniversary of #FlamingJune, I thought I would instead focus on the future. So here goes!
Flaming June 2017! My hopes:
A year is not long in terms of institutional change especially one as large as the NHS. My hope is that by next June we will have developed robust foundations with which to undertake the work to implement the National Maternity review five-year transformation. The NHS England Maternity Transformation board will be up and running, having fully embraced genuine co-design so that women are driving & leading the national changes in maternity services. Women will be embedded top to bottom or rather as I prefer bottom to top, through involvement at all levels via MSLC, MatExp, & other local and national groups. The seven personalisation maternity vanguards will role-model collaborative working with women and families. NHS England will support and strengthen this approach by encouraging sharing of best practice and ideas, linking those areas where women’s leadership and involvement is already embedded with those areas where there is more to do. The transformation board will be promoting cross boundary working across disciplines & geographies with much more emphasis on the need to share good practice so that this is becoming expected routine practice. Every organisation involved in delivery of maternity care will be expected to have a Maternity champion on the board. The National maternity transformation board will support these champions gathering them together to exchange ideas and encourage shared vision and purpose twice yearly.
For a true transformation to occur bravery will be essential. So I hope in a year we will be developing collective bravery. Professionals will need to be brave enough to let go of organisational institutional anxiety, we will need to be thinking about working very differently and we need to acknowledge this will be very difficult for some of us. We will need to support one another and openly listen to those anxieties and difficulties so that we don’t leave people behind. We need to retain quality whilst undergoing transformation, keeping the essentials of safety & experience stable on a background of turbulence. We need to be brave enough to fail. We will need to plan and test innovative co-designed solutions and we will need to learn from this what works and what doesn’t, modify and try again. We need to value and support one another whilst being brave enough to take the opportunity to transform care. If we do this collectively we will be successful.
A key part of the transformation planning will be to focus on individualised care for all women. Women with pre-existing conditions or obstetric complications in pregnancy will not be marginalised or feel discriminated against by the focus on continuity & personalisation. Their need for midwifery support is just as great and they should not be medicalised. Alongside the transformation board, the national programme of improvement of perinatal mental health will be a step closer to being properly funded, with appropriate care provision planned in all areas so that the current postcode lottery is coming to an end. My hope is that maternity and mental health leaders have become well integrated through the regional networks, establishing relationships so that there is more joined-up thinking, treating women and families holistically rather than separating mind and body.
In a year, the Department of Health will have finished a review of funding, recognising the fundamental need for obstetric care, neonatal units, intensive care etc. which carry fixed costs and need properly funding. These costs must not be destabilised by the desire to move to a more community based MDT approach. The DH will have created a viable plan as to how the tariff will work to support the transformation and provided adequate funding for the changes to be sustainable.
To achieve these aims by next June is going to take collective purpose and compassionate leadership. By leadership, I do not just mean those traditional leaders at the top of organisations and departments; everyone has a role to play. Healthcare professionals can recognise and support those who are finding this difficult as well as encourage and enthuse those that are ready for change. How aware are we as a workforce of the changes that are coming? How involved do we feel in shaping those changes? Having those conversations in hospitals, in community clinics on a daily basis will help people see the vision and feel they can help shape the changes. Transformation will become an opportunity and part of our jobs, not a threat externally imposed.
Women and families also have a key role in helping and supporting professionals though conversations either one-on-one or at more formal forums, MSLC, birth forums, maternity networks and so on. When women ask for things staff usually respond, so women have a key role not only in shaping the changes but in supporting and encouraging those trying to implement them. We have already seen this approach work in many ways in #MatExp, women asking for skin-to-skin in theatre or optimal cord clamping are two simple examples.
The National Maternity review itself outlines the need for individual responsibility by both healthcare professionals and the women and families in shaping the future, calling for a grassroots movement to improve maternity care. We are that movement; in a year I want to continue to see #MatExp grow and thrive. We need to continue as individuals taking those little steps and actions every day. Together we can own this change.
With the launch this week of #YourMaternityCare campaign by the Care Quality Commission (CQC) encouraging women to share their maternity experiences now seems as good a time as any to share some of my thinking and importantly ask some questions.
To be clear I am not going to talk scientific methodology, survey design or validity, I am simply going to share some personal ideas as an obstetrician and a member of the #MatExp gang and question if we could use the survey to challenge ourselves in a more creative way.
What sort of impact does this sort of survey have on the care women receive?
The answer to this may depend on how you view the results. It can be examined at a national level looking at care across the country and comparing with previous years to look at trends and themes.
Undoubtedly this survey showed better experiences overall than in previous years and this is good news. An excellent example is the increase in the number of women receiving care before 10 weeks of pregnancy, with a big potential impact on eventual outcome. It is important to take time to give ourselves a collective pat on the back and celebrate those improvements as it can be so easy to focus only on the negatives.
For a great visual overview, take a look at the infographic produced by Picker.
On a regional level the 2013 Maternity survey and the negative results of some London Trusts was actually one of the sparks that led to the London Maternity Strategic Clinical network focusing on ‘Patient experience’. Therefore it directly led to the ‘birth’ of #MatExp and our collaboration with Gill Phillips to produce a maternity version of her Whose Shoes game and development of a workshop toolkit & examples of best practice.
So that’s another positive: the resulting #MatExp change platform and community of people interested in improving maternity experience therefore could be said to be a direct result of the 2013 survey.
We can examine hospital level data and see how a maternity service changes over time, and how women respond on specific questions. This can help us identify a particular area that needs improvement, such as continuity or postnatal care, as well as giving positive feedback about what is working well. It can help us benchmark our services against others locally or nationally. It is undoubtedly a valuable data point even if it has limitations and exclusions however it is only one of many ways we should be looking at feedback.
Most Trusts will have an effective governance system meaning that the results will be reviewed and circulated, an action plan devised and those actions systematically ticked off when completed.
We need to be cautious as it can become all about process and tick boxes if we are not careful, held at management level and a little detached from both those in daily practice and our service users.
I wonder how many Trusts have worked proactively with their Maternity Service Liaison Committee (MSLC), staff and service users since they received their individual 2015 reports to identify what improvements would have the biggest impact for their women and to look at how their survey results correlate with other methods of feedback they use?
Moving on to some specifics now, the very first sentence in the recently published CQC response to the survey results is a shock ‘There are almost 700,000 live births each year in England. Having a baby is the most common reason for a hospital admission.’
Why is this?
According to the National Tariff benchmark data 65% of women are ‘standard’ i.e. do not have a complicated antenatal period and therefore are ‘healthy’ pregnant women.
Therefore, the first challenge from the results is why are so many of these births happening in hospital. It probably has something to do with the fact that the survey showed 63% of women who have given birth previously were definitely given enough information about where to have their baby, falling to 53% of women giving birth for the first time. This presumably means large numbers of women are not getting adequate information.
I’m not going to recap NICE Intrapartum care 190, but we know it provides evidence that for healthy pregnant women who have had a baby before we should be explaining birth at home or in a midwifery led unit is likely to have less intervention and the same outcome as delivery in a hospital.
Across the survey results first time mothers seem to be getting a worse experience with consistently lower results than women who have given birth previously. Is this because we are doing something different for first time mothers, is this because we should be doing something different or is it simply that the different groups of women have different expectations? Do first time mothers have higher expectations and are then disappointed whereas mothers who have given birth previously have lower expectations as they know what it was like last time?
In amongst some good improvement scores remain worrying minorities. 89% of women said that during their antenatal care they were “always” spoken to in a way they could understand – up by 7 percentage points since 2007 (82%). However, this means that 11% were not “always” spoken in this way. 87% of women reported that they were always treated with dignity and respect during labour and birth compared to 85% in 2013, but what about the 13% that were not? Surely these are the fundamental basics of care and should be true for every single woman. What are we doing about these women? Can we identify who they are, are there specific groups we are not catering for or not understanding what they need?
Don’t even get me started on lithotomy: ‘The proportion of women being in a position of lying with legs in stirrups whilst having a normal vaginal delivery has seen a steady increase over the past few years going from 17% in 2010, to 19% in 2013 and 22% in 2015’. What on earth is this all about? In 2015 I undertook a lithotomy challenge on NHS Change day and you can read about my experience in the blog I subsequently wrote.
Postnatal experience is clearly lagging behind antenatal and labour care with much lower figures sitting in the approx. 50% region on all aspects of care including physical and emotional wellbeing. Collectively we need urgent action to address this? But the need for collective action raises a problem. Within the NHS we now have this terrible dilemma collaboration versus competition.
The CQC Response to the survey results clearly highlights Trust who have performed better or worse than expected in the last two surveys. If we accept that these results are valid and not a difference in expectations or different for other reasons, then as a simple solution we could potentially buddy up good performing Trusts with poor performers.
However, Trusts are individual organisations. The strategic clinical networks and NHS England can influence, but there is no obligation for Trusts to help others. If we work at a good Trust what is the incentive to share what works? Pure altruism goes some way, but when you face difficult budget choices and competing demands collaboration can be an easy casualty, and as health care professionals what responsibility do we have to try and improve quality outside our own immediate practice?
I certainly don’t have all the answers. For me #MatExp is some attempt at trying to improve and discuss many of these issues on a broader scale, ignite a lively conversation about maternity care and to encourage others to think that they can influence positive change however big or small.
Florence Wilcock
2016
If you are interested in joining the conversation or taking action on improving maternity experience in anyway jump in and join us on Twitter (find tweets tagged #MatExp), join our group on Facebook, or send us a message.
I had the privilege of hosting one of the weekly #MatExpHour Twitter chats last night, on the topic of “What Does #MatExp Mean To You?” We had already received some thoughts on this topic via the #MatExp Facebook group, and I couldn’t wait to hear what answers we had from the gang on Twitter. I was not disappointed. This campaign that Gill and Flo started has become something more than I think any of us could have imagined. It is with much delight that I share with you what #MatExp means to those involved.
Those who couldn’t make the chat were keen to get in their thoughts in advance:
Emma Jane Sasaru: “To me it embodies what I believe can happen when everyone works together to support families. It means that while many say we cannot improve things we really can. Helen Calvert and I always refer to the starfish story because if we all just make small changes they add up to big change. Always believe you can make a difference because you can.
Personally #MatExp has helped me so much. As many of you know I had PTSD from a terrible birth experience and poor care. #MatExp has given me hope that we can prevent this happening and we can make sure that families are treated with our ‘heart values’. It has helped in my healing, enabled me to meet some amazing people, make changes in my local trust and also further my work to raise awareness around perinatal mental health.
What I love is the passion, the genuine want to improve things for families and the fact that it comes from the heart. Any of you that know Gill and Flo will know this is be true. Thank you everyone and remember you can be the change you want to see.”
Gill was worried about the limitations of Twitter when it came to explaining what #MatExp means to her, but started by sharing this article from The Edge. You don’t have to ask for permission to make change!
Cathy Brewster: “What I love about #MatExp is the coming together of people from diverse backgrounds. As a parent I have been able to directly talk to midwives, obstetricians, commissioners, researchers, MSLCs etc. about homebirth and have gained unique perspective and insights from them all. And I hope they may have gained something useful from me too. #MatExp certainly made it easy for me to get our homebirth posters out there and it is wonderful to see them being used all over the place. The other thing I love about #MatExp is that it’s a platform for learning. It has opened my eyes to so many new maternity issues that I knew nothing about. So a big thank you from me to #MatExp”
Lucy Ruddle: “I found it really useful when I was pregnant, to discuss the choices I had and why certain things were offered / what various hasty discussions with HCPs actually meant etc. So pretty much, a really useful source of good information.”
Susan Parker: “Even though I haven’t been involved for the longest time, for me it’s about parents being able to share their stories and for HCPs to be able to listen and reflect. It’s about sharing information and collaborating. And at times it’s about having a bit of a debate about a certain topic – which is of course a great thing to listen to a different viewpoint that you may not have considered.
On my radar were things like compassionate care, mental health and a mother’s choice. But my eyes have been opened to way more than that because I hadn’t previously experienced those issues, but I can talk to women who have and learn from them. I feel a blog post coming on (but maybe at some point in the future!) would love to do more with #MatExp.”
Michelle’s wonderful blog post about what the Bromley MSLC #WhoseShoes event meant to her can be found here. And Bromley MSLC had got their thoughts in ahead of time:
Have you seen Flo’s amazing Lithotomy Challenge? Read about it here. Amazing to see the people who got involved!
Natalie Finn: “For me it’s knowledge, understanding, support and passion. As an aspiring midwife, I want to extend & broaden my knowledge and there truly is a wealth here. As a mother of 4, I have knowledge of pregnancy/labour/birth, but simply from my perspective and reading others experiences, feedback and action taken interests me immensely. To be a well rounded midwife, I feel I need to see things from all aspects and perspectives, the mothers/families most importantly. Equally my entire maternity experience has been wonderfully positive largely down to having the same wonderful midwife for 6 pregnancies, 2 losses and 4 births over the span of 8 years!! I’m passionate about normalizing birth as a whole as well as home birth, breastfeeding (despite being a reluctant bottle feeding mum!), continuity of care. I also value the level of passion and support shown in this group. No question is too difficult, the cup of #MatExp runs over with understanding and it’s rare to find a community such as this that just so NICE!”
Look what happens when you JFDI! I didn’t ask permission to do the #MatExp Survey!
Gill Phillips made this wonderful film which also demonstrates what #MatExp means to her.
At the end of the day it’s all about women and families.
I was asked to do a talk to student midwives at Salford University last month on the topic of “Women’s Voices” in maternity care. As part of my presentation I included the voices of the midwives who work in maternity care, and a reminder that there are many other women for whom maternity care is their professional, as well as perhaps their personal, experience. “Women’s Voices” in maternity care should cover the midwives, obstetricians, health visitors, doulas who care for us, as well as the women giving birth.
So I decided to start a series of blog posts on “Women’s Voices in #MatExp” from the point of view of those working in maternity, and this is the third of those. This is El Molloy’s experience of supporting breastfeeding. Thank you so much to El for agreeing to write for us.
You can read the first two blogs in the series here and here. And yes, I will be doing a “Men’s Voices in #MatExp” series too. Because this campaign is about all voices.
Helen.x
*********************
I am an NCT Breastfeeding Counsellor in Coventry, and a Peer Supporter on the Infant Feeding Team (run by Coventry City Council). I sit on our local MSLC (Coventry and Rugby CCG) and was a member of the Coventry Breastfeeding Strategy Group. I am also a Babywearing Peer Supporter for Coventry Slings, and am about to do my Consultancy through Slingababy at some point this year. Probably after I finish the dissertation for my MSc in Child Health (through University of Warwick). I also help to facilitate the Coventry NCT Birth Choices (after caesarean or traumatic birth) Group after it was set up and run successfully by one of our amazing local Antenatal Teachers.
This is supposed to be a blog about Breastfeeding Support. Which means it also has to be about being a Peer Supporter – and being a Breastfeeding Counsellor. And now I don’t know who knows what those roles entail, or what we do in either of them. Is there a difference? Can parents tell the difference? Do they care? To be a Peer Supporter, or a Breastfeeding Counsellor – that is the question…I think?
I make a damned good cup of tea (and coffee – because I drink a *lot* of coffee). And at a push I can do cake, but usually I have biscuits. However this is all the icing on the cake or at least bribery, to encourage new mums to come to our groups, have a drink, have a biscuit, and stay a while. Let us listen to your story. And I carry tissues in my bag – always.
As a peer supporter I have had UNICEF training in breastfeeding support (for most projects this is between 6 and 10, 2-hour sessions, delivered by someone who may be the local Infant Feeding Lead Health Visitor or Midwife/IBCLC/NCT Peer Support Trainer). I am a mother who has breastfed her own children. If you want to get technical I *am* a peer supporter – I am still breastfeeding my youngest. I can walk alongside you in your journey, I can tell you that things were and are occasionally tough for me – that despite the official badge and t-shirt (purple this time round, blue before – I declined the hot pink – it clashes with my hair!) I am not an “expert”. I don’t know all the answers – and I’ve yet to meet anyone who does. But as a peer supporter I can tell you what ‘normal’ breastfeeding should look like. I can tell you that there are no rights or wrongs, except what works for you and your baby. With the caveat that baby is happy and you are not in pain. And I can offer you information about what you need to look for in your babies feeding patterns so you can feel confident things are going well.
Does Peer Support make a difference? I’d like to think so – and I can see locally that overwhelmingly most families find us useful. There are always the other stories, the one about the PS who said to use baby rice at 4 months, but that’s no different to the story about the Midwife who said baby should sleep for 4 hours between feeds, or the Health Visitor who suggested controlled crying… One poor piece of information shouldn’t tarnish a whole section of support. This is something we are seeing every day on #MatExp. There is a world of difference between midwives and *this* midwife; between Peer Supporters and *this* Peer Supporter. And the supporters are only ever as good as their training and ongoing Continuing Professional Development (CPD) and supervision.
And this Peer Supporter is also a Breastfeeding Counsellor. Specifically, I am an NCT breastfeeding counsellor. This means, for the uninitiated, that I am trained in person-centred counselling skills, that I am a sign-poster to other information, other options, other Health Care Professionals. But that always the mother is front and centre. This too means that I have breastfed my own children (for a minimum of 6 months – though extenuating circumstances may apply for others). It means that rather than the UNICEF training, I have spent 3 years distance learning through a University accredited course, writing essays, going on weekend workshops. Debriefing my feeding experiences; embedding my counselling skills in practice as well as theory, understanding and training in group facilitation (for both antenatal sessions on courses, and in running breastfeeding groups). Parents aren’t interested in the Diploma that I have, or the ongoing CPD that I have to fulfil, including regular supervision, or the fact that my CPD is specific to each of my roles within NCT. Parents just want to know what I can advise – what I can do to ‘help’. The honest answer is “nothing”. Because in either of my roles, that is not part of my job description. Advising would indicate that, again, I know best – and I do for me, but not for you. I have being trained as a reflective practitioner, and I have recently realised that I have moments of conscious and unconscious competence – I am, as we all are, a work in progress.
If I am visiting you, or welcoming you at our group, I will sit and listen to you talk about your options, and maybe offer suggestions. We might talk about how you feel about what you’re being asked to do, until you come up with a plan that is going to work. Reading the previous blog by Maddie, some of her descriptions about working with parents in labour – asking – what do they want to do, how do they feel… This too is how we work. And the general mistrust by other HCPs feels all too real.
As a peer supporter. I might come to your house on day 1, or day 2 after your discharge. Maybe you called, maybe your midwife referred you because she thinks you need a bit more time, someone to sit while you feed, time that she just hasn’t got because her caseload is so much higher. I fill in forms, I offer to register your child with your local Children’s Centre. I will ask you how your birth was (because this might affect feeding). Maybe your Health Visitor has referred you because you are 12 days in and feeding still isn’t ‘right’ for you. Perhaps your baby still isn’t back to birth weight. We have time. I have time to stay to the end of the feed and see how your baby slips down because the cushion could be in a better place…
As a Breastfeeding Counsellor I also have time to sit and listen to your worries about how feeding didn’t work well with your older child. You might have called me because I facilitated your antenatal session; or maybe you’ve been searching on the internet. You might have called the national line, and they have given you my details. Maybe you have come to the Drop In that I run with another colleague. I might visit you at home, where you apologise for going round in circles about whatever is worrying you – but I sit and listen, and reflect your words to you, or maybe ask the one question, or make the observation, that triggers the understanding in you that your worries are not all feeding related, that you’re concerned about your relationship with your partner.
I too go home and worry; did I say enough, not enough. Did I miss a subtext. I am all too aware of the responsibilities that the midwives and health visitors have. The understaffing, overstretching. We will refer in parents who are struggling. “If you are still concerned talk to your midwife, is this something you feel you can ask your Health Visitor about…”. We will make the phone calls where we are concerned about parents mental health, those feelings where things just feel slightly ‘off’. We trust that you will support families, and we ask that you trust us to do the same. Trust that we have the experience with breastfeeding, that we can and do support mothers long after they stop attending baby weighing clinics, long after their regular assessments – all still breastfeeding. We support them to continue, and to stop when that’s right for them. At 2 months, or 2 years, or even longer.
I want (I want?) I can say it in this context… I want all women to have confidence in their decisions, and to have the right information for them to make the decisions that work for their family. Whether that is because they understand that breastfeeding past 9 months isn’t tantamount to child abuse (yep, that old chestnut); or whether it’s because I signposted her to the information they needed about their anti-depressants which meant they had confidence in continuing to feed even when she felt her world was falling apart. Whether that’s because we worked on positioning until she finally hit that sweet spot and it finally clicked that no, breastfeeding does *not* have to be painful; or whether after seeing 6 other HCPs and being told that she had ‘forgotten’ how painful feeding was, I mentioned tongue tie as another possibility, and lo and behold division did result in huge improvements. We have time, I tell the women I see, don’t worry (often as I’m glancing at the clock, thinking, I’m going to be late to my last visit, and I know that’s 20 minutes away, and it’s already 4.45pm on Friday, and I finish in 30 minutes). When baby won’t latch, or has just fed before I arrived and won’t be woken. “How have things been?” “What have you tried?” “Some parents find…” I joke that all babies sleep for me, except my own. We talk about previous miscarriages, we talk about the joy in feeding her firstborn, and the fear that it won’t work this time. That she’s been told it’s just a “small” tongue tie, but she’s worried about him swallowing blood; we talk about how to deal with engorgement, and how can she ease the cramps that accompany her let down. How can her partner bond with baby, so when can she start expressing; we talk about shared bath times, and babywearing. And how will she cope when he goes back to work. We have such a fluid society that we don’t often live close to our mothers, and can’t learn from them the way we used to. My visits span the world, from South Africa to Vietnam, to Latvia, Canada or Scotland. The accents change but the worries and fears are all the same.
It gets easier, you can do this. And particularly in the light of the media frenzy unleashed by the Breastfeeding Series published by the Lancet. We can do this. Together we can change the world.
I was asked to do a talk to student midwives at Salford University this month on the topic of “Women’s Voices” in maternity care. As part of my presentation I included the voices of the midwives who work in maternity care, and a reminder that there are many other women for whom maternity care is their professional, as well as perhaps their personal, experience. “Women’s Voices” in maternity care should cover the midwives, obstetricians, health visitors, doulas who care for us, as well as the women giving birth.
So I decided to start a series of blog posts on “Women’s Voices in #MatExp” from the point of view of those working in maternity, and this is the second of those. This is Maddie McMahon’s experience of being a doula. Thank you so much to Maddie for agreeing to write for us.
You can read the first blog in the series here. And yes, I will be doing a “Men’s Voices in #MatExp” series too. Because this campaign is about all voices.
Helen.x
*********************
Maddie McMahon is a doula, doula mentor, doula course leader and breastfeeding counsellor in Cambridge. She is also a member of the board of Doula UK. She supports women using the same hospital she, herself, gave birth in and has been a staunch supporter of that hospital ever since, sitting on the MSLC since 2004.
She is author of ‘Why Doulas Matter’, published by Pinter & Martin in 2015.
I have been a doula for 13 years and have supported hundreds of women, either before their birthing, during their labours or afterwards. I have been facilitating an initial doula preparation course since 2008 and have been mentoring doulas and intimately involved in the evolution of the doula community in Britain since early on in the history of Doula UK.
In all those years I have learned more about what a doula is not, than what a doula is. Every time I think I might have got a handle on the ‘definition of a doula’, my understanding and perception shifts again. The definitions that do the rounds on the internet can be shallow, to say the least and, at best, undermining and dismissive of the incredible talents and abilities that women bring to this role.
I see all sorts of women being called to serve the mothers of their communities. There are women, like me, who felt a gaping hole or a contrast in how the time of transition into motherhood can feel so very different with and without psycho-social support.
There are women who feel betrayed and let down by their health professionals. They may be fighting birth trauma or PTSD or just a deep sadness.
But there are also mothers joining the community now who have been supported by a doula themselves, feel ecstatic about their birth experience and have been inspired to pay it forward.
There are women who, despite all their protestations of loyalty to their careers, found that motherhood remade them, in a fundamental way, bringing them to a realisation that ‘work’ needs to fit around children, nurture our souls and service our communities if it is to be truly worthwhile.
Some come to the role from an academic direction. They are incredibly bright PhD students or researchers, for example. They are interested in motherhood from a sociological, anthropological, political, psychological or philosophical standpoint. They may be activists or campaigners.
Then there are the Human Rights doulas, the ones interested in things like consent, maternal rights and responsibilities. They may have worked in sex and relationship education, or in women’s advocacy or legal settings.
Related, are the doulas who come to the work through their work with social services, or other support of vulnerable or hard-to-reach groups. I know many doulas who started off working with Birth Companions, working with women in prison, or as Homestart volunteers, in teenage pregnancy units, or are Maternity Support Workers..
And there are those who see birth as merely one step on a female journey, all of which deserve emotional and practical support. They support their community of women through menarche, marriage and divorce, abortion and baby loss, birth, breastfeeding and beyond, right up to menopause and sometimes doula families through the last and ultimate transition – death.. They are the white witches, the humanists and the pagans, the searchers for and creators of ritual and ceremony, the red tent facilitators, the women’s circle founders…
The ‘breastfeeding doulas’, through their voluntary work as breastfeeding counsellors, come to see that the challenges women face initiating and maintaining breastfeeding are often down to wider social and familial pressures. They begin to see these pressures and understand that, much as we can suggest to women to go home, sit and enjoy nursing their newborn, it doesn’t magically get the washing up done. The hour they can spend with women in the breastfeeding clinic doesn’t give them the space and time to explore the social attitudes that invisibly pressurise them to supplement with formula, or sleep train, or help their partner take a more active interest in the baby.
Related are the ‘babywearing doulas’ and the nanny and childminder doulas who, again, have come to the work through close contact with new mothers…who have seen close up that mothers of newborns need a particular type of peer support that the doula ethos perfectly encompasses – that time, and space we can give. That unconditional listening ear. That ability to help a mother access and trust her own mothering instincts. The way a doula supports a mother to do the mothering, and supports the partner/father too to step up and find his skills and abilities as a parent. The doula way of somehow ‘de-medicalising’ motherhood.
And lastly, but certainly not least there are the midwives. Some are retiring. Some have been out of the midwifery loop for a while and are choosing between a return to practice course or the doula route. Others are, quite literally and very sadly, at the end of their tether with the NHS and the constraints it places on midwives and mothers. They often feel like they can’t practice in the way they would so love to; supporting women through the whole journey. Continuity of care, pressure to follow guidelines and management that pays mere lip service to issues like individualised care, consent and compassionate care, have driven them to throw in the towel.
As you can see, many of these women might be bringing baggage to the role. They may well have conscious or unconscious axes to to grind. It is through doing a doula course that we aim to create a safe space to process and contain this baggage, to become conscious of our worldview and how it might create the version we see of the world. We begin to practice ways to bring ourselves back to the women and families we serve, to see the world through their eyes and to therefore support them unconditionally and without judgement. Because it is this lack of an agenda, a lack of micro-managing guidelines and regulations that allow families to relax into our presence and for doulas to become a trusted part of the family.
All experienced doulas know that we are, in some respects, extremely lucky. We revel in the luxury of not having to follow guidelines, merely supported by the philosophy and Code of Conduct that our community has created for itself. We are free to build deep and abiding relationships with women, their partners and their children. We get to listen to her deepest fears and anxieties, support her to find solutions to her practical challenges and gain a deep understanding of her desires for this birth and beyond. We never, ever make the mistake of assuming that women might hold the experience of childbirth above the safety of themselves and their babies. Every working day teaches us that this idea is ludicrous. We see the birth trauma, the family dynamics, the physical and mental challenges that explain a woman’s choices. Really, really close up, it all, always, makes sense.
So, we have this deep, vital knowledge of a woman and why she wants what she wants. We have seen her do her research, read studies, talk to professionals, lay/peer supporters, friends and family. She has worked it through in her mind and her heart. She understands the risks and benefits of the choices she is making. We walk with her on this journey, every step of the way. So, when that journey gets to the point where we might be sharing a space with midwives or obstetricians, we have to seamlessly move from being a team of 2 or 3 and move aside in a loving way to bring these professionals into the circle so that we can create a loving circle around the woman.
That dance can go in a number of different directions, depending on the circumstances. There are some common challenges that can prevent good relations between doulas and staff in the birth room. One of them is possessiveness on the part of the doula. It’s wrong, and egotistical and something that shrivels as she gets more experienced, but I do think we can be forgiven, just a little bit, for thinking that we know better than the maternity staff what the woman wants and needs. It can make us a little defensive when they appear not to have read her birth wishes. It can make us a little grumpy when someone comes into an atmosphere that we have set up according to her wishes and switch on the lights and start talking loudly.
Perhaps we aren’t always super-skilled at handling those kinds of interactions. And perhaps there is more going in underneath those interactions than we doulas are sometimes aware of. If I ask if it’s possible for us to find a floor mat for a labouring woman, and that midwife has just been having a conversation with a colleague about doulas and how we have a ‘natural birth and all costs’ agenda, she may read more into my request than I intended.
If a VBAC couple ask a doula to tell the midwife they don’t want continuous monitoring, how can that be handled? The midwife may not know that they have done their research antenatally and made an informed decision. She may wonder who the hell this doula is, who appears to be talking for the couple. How does a midwife know that these parents aren’t being coerced or persuaded into a course of action without understanding all the possible ramifications? How does that midwife know she will be supported by her colleagues to support this ‘off-piste’ decision?
Sometimes we are aware that there is an underlying atmosphere in the room based on these myths and misunderstandings about a doula’s role. Most of us have realised that it’s common for midwives to think that all doulas are frustrated, wanna-be midwives. Some think we meet the clients for the first time when they are in labour. Many think we are making an inordinate amount of money. Some see the intimate connection we have with the couple and are forced to contemplate why they, themselves were drawn to birthwork in the first place and how it hasn’t quite turned out the way they longed for.
Other times, when a member of the obstetric staff is in the room, the presence of a doula can wrong-foot and confuddle them no end. They are talking to a couple, counselling them through their options, and they suddenly turn to the anonymous, unnoticed woman in the corner, and ask her what she thinks. Even more confusingly, sometimes she asks a question that sounds surprisingly knowledgeable, or asks the couple if they need anymore information about the risks and benefits, or wonders whether there is an option to do nothing at all. She may suggest a few minutes of alone time to think and usher everyone out of the room. The woman they assumed to be Auntie Doris, is suddenly orchestrating the situation somewhat. Unsettling to say the least. Worrying, perhaps, and possibly anger-inducing.
After the baby is born and a community midwife or Health Visitor visits, it can be hard for her, in the time allowed for the visit, to get a real handle on who this woman is who appears to know her way around the kitchen and hangs around in the same room for the duration of the visit. Can the mother talk freely in front of her? Is the doula giving out of date or wrong baby care or breastfeeding advice? These concerns remain unsaid, but can prevent a real human connection.
We know that sometimes, both doulas and staff bring baggage, myths and ignorance of each other’s roles into the birth room. And most of the time, it is our communication skills, or lack on them, that prevent a deeper affinity and closer working practices developing.
All those talented women, with enormous hearts and the energy to support birth, whether they are clinical or lay, deserve to have the love and support of each other. We all have a massive amount to give.
Doulas are responsible for some of the most positive support networks in recent times: The Positive Birth Movement (PBM), Birthrights, the VBAC and Birth Choices support groups, social media support, breastfeeding support to name but a few. When those support networks work most beautifully is when lay women and midwives work together as equals, loving and respecting the complementary threads we each bring to the work. By working alongside each other, we both learn and grow, for the benefit of the mothers we support.
These communities we build, the rituals we rebirth – these are the special and truly valuable aspects of the doula movement. Perhaps now is the time to validate this grassroots work and build on the models we have set up, that are clearly spectacularly successful! 170 PBM groups in the UK alone. 40,000 followers of Dispelling Breastfeeding Myths on Facebook, 10,000 followers of Birthrights. Community support and advocacy is clearly needed – in fact women are hungry for it. And a lot of this community-building work is about supporting health professionals too. Many doulas work to provide community support to their local student midwives, or welcome community midwives to their mother-support groups. We raise money for our local hospitals, sit on MSLCs, try to raise awareness of the challenges facing maternity services, even march alongside them, with placards raised.
We like to think of the mother, at the centre, as the sun, with her supporters orbiting around her in elliptical trajectories. Sometimes the midwife moves in closer, sometimes the doula or the doctor. We move further away to make space, to allow the mother room to make decisions and find her own answers. We move in closer when she needs physical or emotional support. We recognise each other’s skills and talents and make way for each gift to be bestowed with love and appropriacy.
When we all work more closely together, we see for ourselves how much the doula philosophy of information without agenda, unconditional emotional support and listening without giving advice have a tangible effect on outcomes – not just in birth statistics but on the mother’s state of mind and her emotional and physical ability to mother her infant.
Many doulas know that some of us could learn a little more humbleness from midwives and Obs and understand a little more quite how challenging, heart-breaking and downright soul destroying their work can be sometimes. And perhaps they could learn a little from us – about compassionate listening and keeping care woman-centred, tailored to her personality, preferences and anxieties. They could learn how our depth of relationship with a family may give us insights they don’t have, and not to feel defensive about that, or jealous.
So how can be build better understanding and cooperative working practices?
We see a lot of wonderful stuff going on already: doulas being asked to meet and speak with student midwives, so that they learn about our role from the beginning. It would be good if this were extended to student doctors too.
Some doula preparation courses will allow midwives and student midwives to sit in, for free – to get a taste of the doula community and an in-depth understanding of the many variations of the doula role.
Many doulas sit on MSLCs and Labour Ward Forums, which is a great way for us to share stories and client experiences and to learn more about the workings of the service and the challenges it faces. Mutual empathy is often very effectively built this way. It can work even better when the staff come out to sit in our forums – to visit our pregnancy support, breastfeeding and parenting support groups.
Social media is one way forward. The relationships and mutual respect between doulas and midwives has blossomed since we have begun to get to know each other on Facebook and twitter. We can really help each other – doulas helping the campaign to spread the knowledge of Optimal Cord Clamping springs to mind, or spreading understanding and therefore driving consumer demand for the ‘gentle’ or ‘woman-centred’ caesarean and ‘seeding the microbiome’. We are also able to provide each other with emotional support online and these friendships sometimes benefit mothers in very tangible, ‘I know exactly the right person for you to talk to’ kind of way.
We’d like to see us working together to create more models that provide psycho-social support for more vulnerable and hard-to-reach groups. That 14 year old girl may well have a wonderful specialist midwife to support her, and perhaps the young parents group at the local children’s centre to tap into. But wouldn’t it be wonderful to find out whether any of the local doulas have experience in this area or were young mothers themselves? Sometimes someone coming along who isn’t wearing a badge or a uniform, can make all the difference.
What about those women who ask for elective c-sections with no clinical indication? How many units have specialist counselling services for tokophobia or birth trauma? How many doctors or midwives suggest to women that a bit of peer support might help? Signposting to ‘patient support groups’ can make all the difference, as many women’s accounts of the effect of other mother’s positive stories attest.
There are doulas who have experience of working with women in prison, doulas who are also clinical psychologists, doulas who work exclusively with young mothers, or who work closely with Social Services or Homestart. There are doulas who have a lot of experience building rapport and trust with women who are suffering huge anxiety, and doulas who work with women with particular conditions, like Hyperemesis. There are doulas who specialise in breastfeeding support and who are also Breastfeeding Counsellors or IBCLCs.
Some of us receive direct referrals from maternity staff. Some don’t. Some hospitals have built formal, cooperative models that incorporate doulas, in a voluntary or paid capacity, into the system in some way. Sharing best practice, spreading ideas, building on the successes and working sustainability, mutual knowledge sharing and auditing into the processes seems to us to be the way forward.
Given that doula support appears to have a growing body of evidence to suggest we can increase normal birth rates, minimise cesarean sections and save the NHS money, it is surely time to begin to formalise our partnerships.
So if you are a health professional, why not resolve to find out about the doulas in your area? Perhaps invite them for a cup of tea – they’ll bring the cake.
This post is from Michelle Quashie, and originally appeared on her blog site Strong Since Birth. Our thanks to Michelle for agreeing for it to be reposted here.
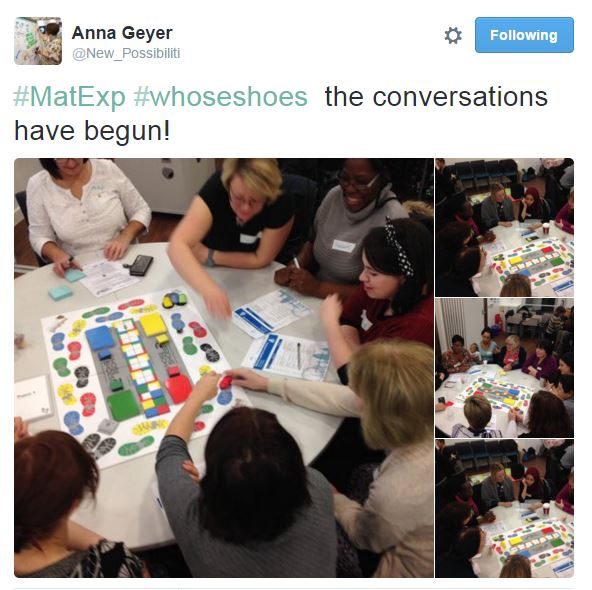
The day had finally arrived! After contributing to #MatExp and interacting with many conversations surrounding ‘WhoseShoes’ throughout the year, I was finally going to experience the magic in real life.
Laura, the chair of our MSLC has written a fantastic post that captures the excitement of the day perfectly, you can read it here: When WhoseShoes Came To The PRUH
I was not disappointed, the day was everything I had dreamed of, but for me it was so much more.
I was asked to open the event by sharing my Maternity Experience. I have spoke at several maternity training events in the past but my audience has always been Midwives. I was aware that this was a multi discipline training event and it was to be the first time I would share my story in such detail with Obstetricians and everyone else involved in Maternity. The thought made me feel anxious but I knew how important this opportunity was.
I had planned to stay in control and not let the emotions attached to my experience be displayed in the form of tears. It was so important to me to remain composed and in control.
My heart pounded through the showing of the MatExp film, this film moves me every time. It is so powerful and very thought provoking. Sadly I can resonate with many of the situations displayed in the film. I knew I was about to be discussing some of those memories any minute with all those surrounding me.
My name was called and I made my way to the front with my heart pounding. I decided to be honest and share how I was feeling with the room.
‘Please bare with me, I am feeling very nervous. I’m sure once I start talking I will warm up and I will be fine!’
Automatically I felt more relaxed and felt more able to share my story without the anxiety overruling my thoughts.
It’s amazing how every time I share my experience it comes out slightly different, or I find myself saying things that I hadn’t thought of before? I had missed a couple of important bits out but neither the less I was very happy with the way I had presented and gauging by the feeling of emotion in the room I had touched the hearts of nearly everyone around me. For the first time I was able to keep my tears to myself even though I had noted that tears were shed by many in response. The room fell silent but the atmosphere spoke volumes.
I wasn’t aware of the tweets that were being circulated on social media but looking at them them later along with the emails I had received It confirmed that my talk was a positive part of the day.
“Also a massive well done to Michelle for her heartfelt and emotional story, I could see it touched many people as there were certainly a few tears in the room. That took huge courage to stand there in front of so many people and share such a personal experience and to tell it so well. Huge WELL DONE Michelle.”
We began to play the the game and interesting discussions were had in response to the thought provoking questions that are key to the WhoseShoes success.
Some of the discussions that stick in my mind were:
A woman wanted a home birth but her husband wasn’t convinced. We had discussed that there wasn’t enough support or information given during antenatal care to ensure that the couple felt safe,supported and empowered to fulfil the woman’s birth choice.
Consultant Obstetricians are normally addressed by other members of their team using their title i.e., Sir, Mr, Mrs or Miss as a mark of respect. I may be wrong but it feels hierarchical, unlike the power slogan and barrier breaker behind WhoseShoes and #MatExp ‘No Hierarchy, just ordinary people’.
It was also discussed that consultants were on site until 9 pm, after that they are on call for emergency situations only. Now I understand why during my appointment to discuss my VBAC, the registrar said ‘ I mean, we don’t know when you will go into labour or who will be on duty should you rupture’. I now understand that my birth choices were influenced by staffing levels at the hospital.
Other key themes were Empathy, Language, supporting and facilitating informed decision making and just how important it was for everyone to be cared for individually based on their individual situation and needs.
Midwives are able to have time to build a relationship with women whereas doctors are often called for the emergency situation and do their best to resolve the medical issue as it arises. This can sometimes make it hard for them to be able to connect with the woman that they are caring for and are not always able to fully appreciate the long lasting effects the experience can have on a woman.
The day was coming to an end and Anna gave us fabulous evaluation of our morning using the comments that came from the discussion at each table. It was fabulous to visualise the discussion using the graphic that Anna had been working on through out the morning.
We each made an individual pledges. Here is my pledge:
“To provide a platform for women to share their Maternity experience. I would like to ensure that women’s voices are heard as part of training and development.”
I am currently planning a conference called ‘Women’s Voices’. More details will be available soon.
As the morning came to an end and people were leaving someone tapped me on my shoulder. I turned round and my tummy flipped. The face before me took me straight to a place of feeling vulnerable, feeling panicky.
‘Michelle it was me wasn’t it?’
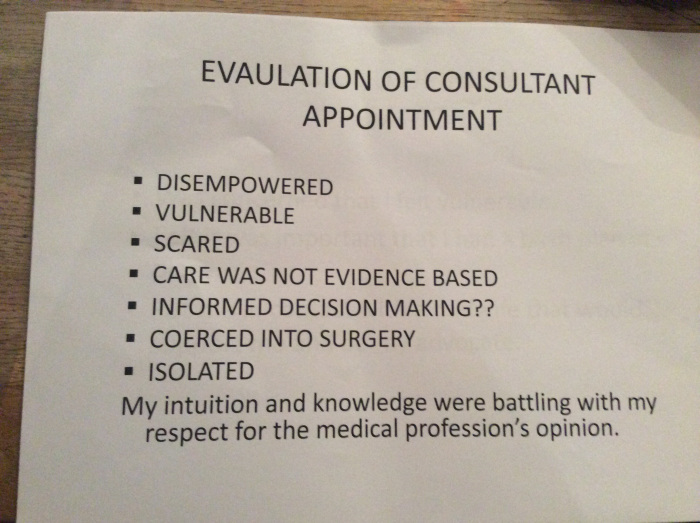
Stood before me was the registrar that I had my consultation for my vba2c with. Unbeknown to my self and the organisers we had shared the morning. I had shared an experience that changed my life but had also been a time that left me feeling scared, vulnerable, isolated and questioning my mental health. The person that was responsible for those feelings was standing here in front of me, for a moment the feelings came flooding back, I battled to keep them contained.
She apologised for the way she had cared for me. She admitted that she had been wrong and has since ensured that she was fully aware of her professional guidance. She was now fully supportive of women’s choice regarding their birth and ensured me that since having to write a statement in response to my complaint, she is fully aware of the impact of the care she provides a woman.
She actually thanked me for highlighting the error of her ways promising me it had changed her attitudes. I could see that she was overwhelmed with emotion and had spoke to me honestly. She asked if she could hug me and we both held each other for comfort.
I told her that I admired her for taking the time to come a talk to me and for apologising. I also explained that I was aware that she was not entirely to blame for the care I had received and I now understood that her response to me wanting a vaginal birth after two caesareans was due to the cultural belief of the trust she worked in.
It was clear that my birth wishes would not be supported and neither would anyone wanting to support me at that time. I know this because many attempts were made to provide me with the support I needed and no one stepped out of their comfort zone to provide me with the support I needed with regards me birth choices. As a result I had no choice but to transfer my care.
She empathised and promised me that as a result of my experience things were changing.
We said our goodbyes and I was trying very hard to contain my emotion that the meeting had evoked.
A consultant midwife that has walked by my side through this maternity experience and others and who has been a pillar of support to me came to see me. ‘Are you OK Michelle?’
The flood gates open and I broke down. I couldn’t talk at that moment. I was just overwhelmed with emotion. I couldn’t make sense of it at the time but now I think I can.
That meeting with the registrar brought some closure. I admire her ability to acknowledge the error of her ways.
The meeting took me back and reminded me of the scared women I once was sitting in her office, trying to persuade her that I could give birth, pleading with them to allow me. Feeling so horrible when it was highlighted that I had never given birth and they wasn’t sure if I could. I was subjected to a number of negative comments that effected my mental well being and left me questioning my sanity. Comments that left my family feeling unable to support my decisions in fear of my safety. it was a meeting that left me feeling isolated.
Here I sat after coming full circle with the same women but this time I was a different woman. I am a now a woman who has had the most amazing journey and have achieved some incredible things;
I gave birth, not only did I give birth but I bloody rocked that labour ward!
I came back and I told the story, I sang it from the rooftops!
I learnt to believe in me and my abilities.
I joined their MSLC and contributed to so many fantastic improvements within the Maternity service.
I have spoke at training events within maternity with an aim to improve maternity care for women.
I have written and had my views published here and in The Practising Midwife .
I have contributed to #MatExp campaign and connected with some fantastic people as a result.
I have met, received support and been inspired by many fantastic people. too many to mention.
The realisation that my shoes have climbed a mountain has happened!
I received the following email from a Consultant Obstetrician following the Whose Shoes event. It confirmed that this journey has been worth every little step:
“Dear Michelle,
I just wanted to reiterate how touched I was by your story and how impressed I was by the way you delivered it. You will be responsible for improving the practise of every obstetrician in that room today which in the end will improve the care of tens of thousands of women.
Having observed the Guys and St. Thomas’s event in the summer of 2015, I knew we were in for a treat. I hoped and prayed that our event would generate a similar level of commitment that was felt at Guys, and I was not disappointed.
50 delegates, representing midwives, maternity support workers, doctors, commissioners, service users, receptionists, porters, health visitors and many other areas of maternity, streamed into the Education Centre promptly at 9:30. The day was introduced by Maxine Spencer, director of midwifery, who spoke about the day being a level playing field and that everyone was there as a mother, a wife, a sister, a daughter (or a father or son for the men in the room), irrespective of their profession.
Having watched the “In their Shoes” MatExp DVD, during which you could have heard a pin drop, it was then the turn of service user Michelle Quashie to tell us her VBA2C experience. Again, everyone listened with respect and focus and there were tears from a few as she retold her powerful and inspirational story.
After everyone had composed themselves, it was time for the game to begin. Conversations started off fairly hesitantly, but people warmed up and pretty soon it was obvious how powerful this day would be.
On our table discussions ranged from noise on the postnatal wards, to caring for staff and teamwork, how to support women’s feeding choices and the power of language. Everyone spoke in a respectful manner and was very honest and open. Conversations just flowed and, as a facilitator, it was wonderful to see how professionals often spoke from the heart as service users. Proof that birth matters to everyone.
The wonderful Anna Geyer from New Possibilities weaved her magic on the plethora of post-it notes being generated from the discussions and as usual created the most beautiful graphic.
Tweeting was fast and furious during the day, to the point where I thought my Twitter feed was going to explode! Here are just a few of the hundreds of tweets:
Eventually, after a couple of hours, the discussions were brought to a close and Anna gave us her evaluation of the day, drawing out some of the points that we had raised.
As chair of Bromley MSLC, I was delighted to see the weight attached to having a strong, powerful MSLC as a voice for service users and professionals alike.
Then it was time for the pledges. Each individual was invited to pledge one thing that they would do differently as a result of attending the morning. Spontaneously, everyone clapped and cheered as one pledge from each table was read out. I haven’t had time to go through them all yet, but here are a handful that stood out:
“I will try to make every birth special (in theatre especially)”
“I will not use the following words: allow, only and let”
“To try and make the ward round more personal, friendly and positive and a respectful experience for the woman and her family”
“To always ask how the new father is as well as the new mother”
“I will facilitate a “good news” newsletter and encourage all staff to submit thank yous and nominate staff for good support”
“I will ensure that I always remember to update the woman and relatives on what is going on”
“I will make sure that every woman feels had the attention and care she hoped for”
“I will always say hello and congratulate all new parents on the ward”
“I will continue to facilitate named midwives (and ensure that) a woman sees her named midwife at least 4 times during her pregnancy.”
“To provide a platform for women to share their maternity experiences”
What now?
The Bromley MSLC has gathered together all these pledges, which will form our work plan for the next 12 months or so. We intend to monitor and check that they are being implemented. Amazingly, by the time I’d returned home and fired up my computer, one staff member had already emailed her colleagues to initiate the first “good news” newsletter. THAT is MatExp in action!!!
The other email in my inbox when I returned was from a service user who had attended the day. She asked me to share this with other members of the MSLC. She said:
I just wanted to express my thanks and congratulations on your amazing achievement on getting today’s ‘Whose shoes’ event to actually happen and to everyone else who was involved in organising this outstanding event.
What an absolutely amazing experience it was and so refreshing to see such a mix of service users and professionals all come together, to share knowledge and stories and all with the same goal, of making a difference to our maternity services.
I thoroughly enjoyed the morning and could have easily carried on for the rest of the day!!!
As discussed today on my table, people are very quick to complain, but never quick to praise so I thought I would come home and express my feelings and give my praise.
So thank you and I will see lots of you at the MSLC meeting next week. Really looking forward to seeing what the year ahead holds now we have our pledges to work with!!
I was fairly certain we were in for a special day, but I was overjoyed to feel the tangible buzz and energy created in the room. It was a privilege to witness how something so simple; getting professionals and parents together to talk about improving maternity services in a compassionate, respectful manner, can have such an impact. From the number of comments I’ve had flood into my inbox in the last 24 hours, I think its safe to say that everyone came away feeling fired up and committed to making local maternity services the best they can possibly be. I know it renewed my enthusiasm to do just that.
Oh, and one final thing. I think we raised the stakes of the #MatExp #bakeoff challenge!
Personally I have had a bit of a Christmas and New Year break, but of course #MatExp never sleeps! There have been plenty of blogs, new ideas, events planned and meet ups occurring all over the festive period. We have had new people join the Facebook group, new ideas suggested for #MatExpHour and lots of us are speaking at events around the country in the coming weeks and months.
It seems five minutes since the fantastic #MatExpAdvent initiative came to an end, but here we are on the eleventh day of 2016 and I need to dive back in as otherwise I’ll be left behind! This wonderful round up from Gill Phillips inspired me this morning to get back on the crazy horse…..
Our last #MatExpHour before Christmas, led by the wonderful 23weeksocks, was on the topic of Taking #MatExp Into 2016. There were some excellent suggestions for actions and initiatives, so let’s take a look and then get cracking! What would you like to do?
The NCT has developed a new practical guide to running an Maternity Services Liaison Committee (MSLC), “From Good Practice to Trouble Shooting”. MSLCs are a big part of #MatExp, and there are some exciting WhoseShoes #MatExp MSLC events coming up very soon!
Are you already a member of an MSLC? What has your group got planned for this year? Is there an MSLC in your area that you can join? Definitely a lot going on around the country – let us know how #MatExp can support your MSLC, joining hands around the country!
It was also suggested that #MatExp could work more closely with the fantastic 1001 Critical Days campaign.
Are you involved with this project? How can #MatExp best support the campaign, and vice versa? Do you have some fresh ideas about the conception to age 2 period? We have many Health Visitors involved in #MatExp and their input here will be invaluable.
The next suggestion was harnessing the power of the next generation of midwives via the country’s Midwifery Societies. Are you a member of a MidSoc? How can you collaborate with #MatExp? Could you host a WhoseShoes event? Do you have events coming up where #MatExp could be represented? What is on your agenda for 2016?
My aim for 2016 is to try to take #MatExp to those not on social media. How do we engage with healthcare professionals (and parents) who are not on Twitter and Facebook? Looks like we will have to resort to good old fashioned pen and paper! Or at least keyboard and printer. Who in your trust would you like to tell about #MatExp? Get in touch and help me to spread the message further!
The big thing we are all waiting for is the report from the National Maternity Review. At the Birth Tank 2 event Baroness Cumberlege had hoped that it would be published on 31 December 2015, but unfortunately it is not yet available. Once it is here we can get stuck in with implementing recommendations at a local level.
And what else have people suggested? #MatExp is about all voices, everyone getting stuck in doing what they can, when they can, where they can. A few more ideas to get you inspired:
Anyone wanting to order #MatExp stickers and other resources can do so here.
What’s your plan? What is happening in your area? What needs to be done? What can be built upon? Who needs to be involved? What small things can you do? What BIG things can you do? Whatever you are up to remember to tell us on Twitter at hashtag #MatExp, join in on Facebook, comment on this blog post, send us a message by carrier pigeon, write it on the sky….. The #MatExp train is steaming down the track. All aboard for 2016!