Being in a healthcare environment – whether that be a GP’s surgery or a hospital – can be a hugely disempowering experience. You are likely to feel especially disempowered when you receive bad news – your head spinning, struggling to take in usually complex information. Then, more than ever healthcare professionals of all disciplines need to reflect that each patient is an individual, with their own experiences, values, hopes and fears.
Professionals need to be able to listen effectively, which includes reflecting back what a patient has said to check their understanding, and to make sure they understand a patient’s views.
My son Hugo was born 16 weeks prematurely because I had the life-threatening pregnancy conditions HELLP syndrome and pre-eclampsia. My beautiful boy fought so hard, but died in my arms at the age of 35 days.
Everything possible was done to save Hugo’s life. Sadly, he was too small, and too premature.
There were, however, areas of both mine and Hugo’s care that could have been better. These issues were around communication – there were occasions where stresses could have been avoided if there had been better interaction between staff, or if we had been provided with more suitable written information.
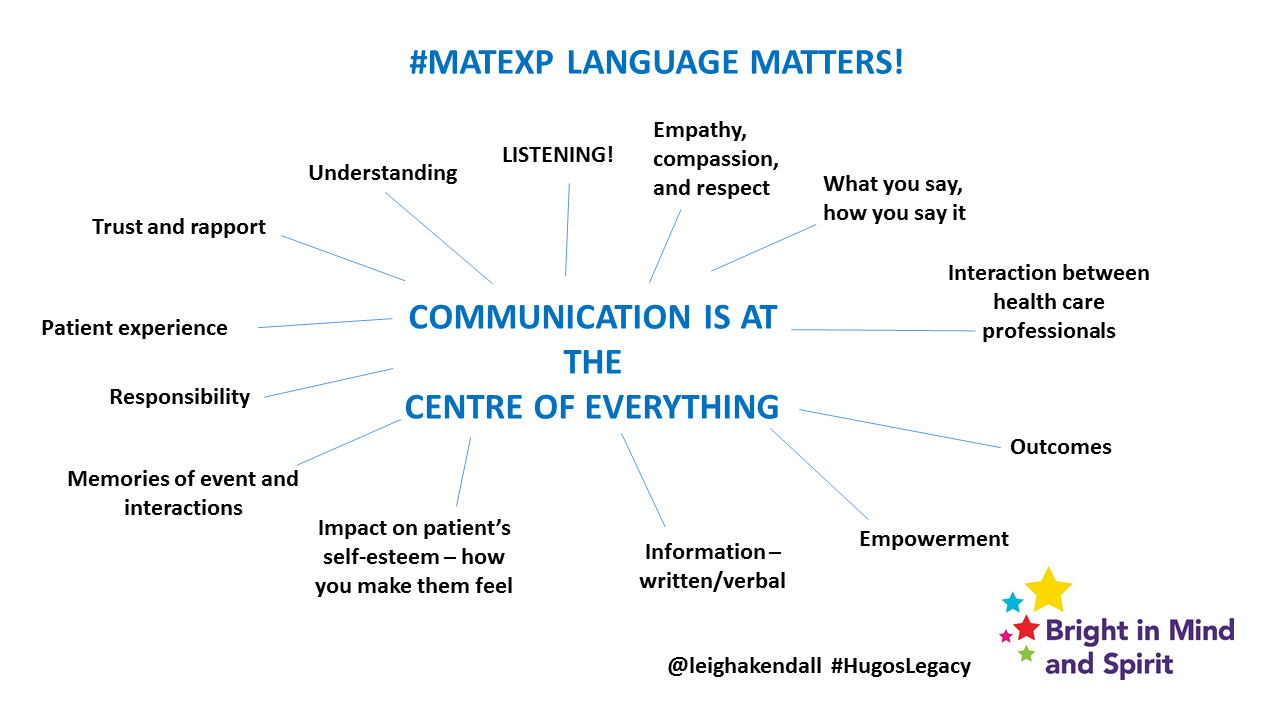
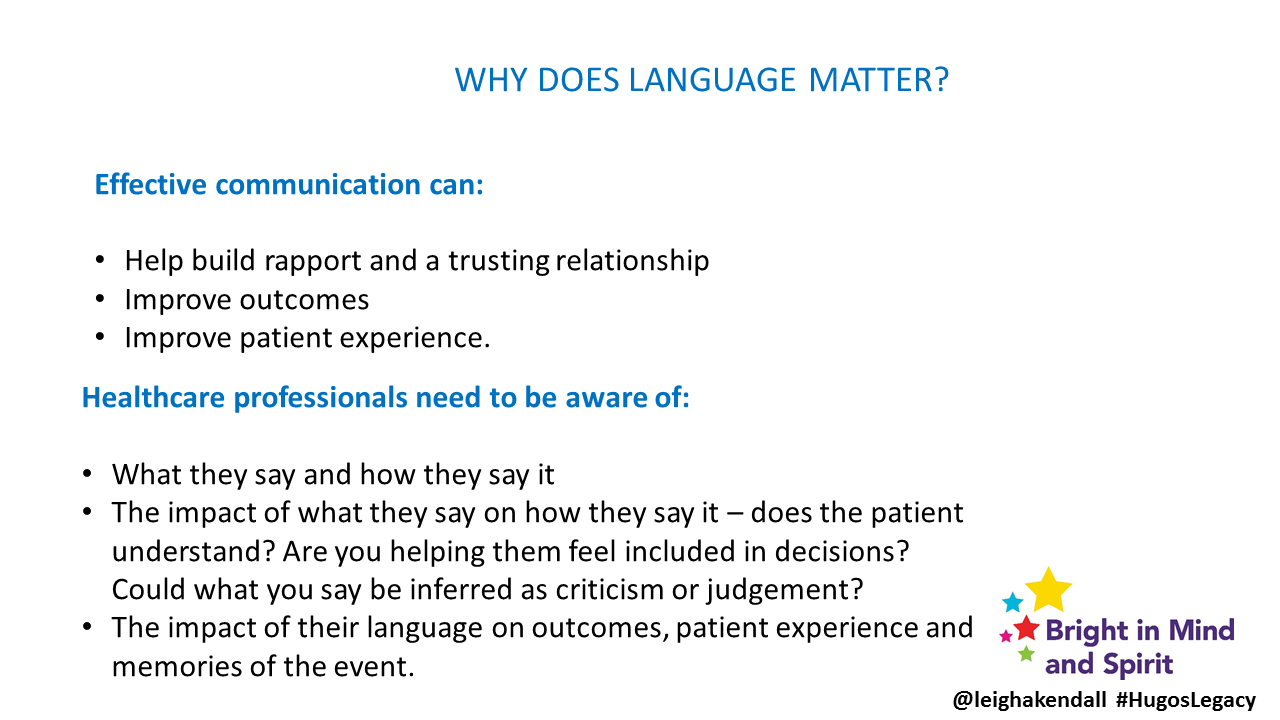
I’m proud to be the #MatExp language champion. Effective language and communication underpins so much, and even a few thoughtless words can cause enduring hurt.
A huge thank you is owed to everyone who shared this post asking parents to get in touch about their own communication experiences around baby loss. An even greater debt of gratitude is owed to those who got in touch to share their experiences – good and bad.
It was interesting that the bad experiences reflected what I suspected – they are focused around failing to reflect that each patient is an individual, with their own hopes and dreams. The incidences of good communication are heartening.
I will take the poor first, so we can end on a positive note with the good.
One mother had a medical termination because her baby was diagnosed with a condition that meant they sadly would not live. I was appalled at what the mum had to say:
We were ushered in to see a male consultant. He obviously did not have adequate time to spend with us. Everything he said felt like one more thing he had to tick off his to do list. His comment: “at this point, I have to say that I’m sorry for your loss” was the least genuine and sympathetic expression I have ever heard in my life. He then followed this by referring to our baby, OUR BABY, as the “retained product of conception” and the loss of our baby, THE LOSS, as “the event”. He sickened me!
Another mum said:
…we had decided to have an amnio. We explained this to the Community Midwife (whose first words as we walked in was ‘oh this will be an easy appointment’….how little she knew!) Her response? ‘But how would you feel if you lost it and nothing was wrong’ said in a very judgemental way. As if we had not consider the risks…..I left the appointment gobsmacked she could be so insensitive and was so upset, I sobbed all the way home.
A woman who had a miscarriage said:
He then flippantly answered my questions in a nonsensical fashion. “It would hurt no more than a period” (I found labour easier, was offered pethidine for the pain all whilst being physically sick). “I wouldn’t need to stay the night” (ummm…I did…. “I wouldn’t bleed much” (not true). And my personal favourite: “no, you don’t need any medication now. Go home and just turn up at any point on Friday and we’ll deal with you.” (15 minutes later and in a taxi on our way home I noticed numerous missed calls. As we thought, I had needed to take the first of my tablets and was asked to return to the hospital as soon as possible.)
The two examples around my own experience include when discussing Hugo’s end of life, in my distress I cried how guilty I felt. The consultant said:
All mothers feel guilty.
That may be so – no mother of a premature baby, or a baby that dies for whatever reason is at fault. Knowing that does not diminish our sense of guilt, and that comment felt very dismissive. I wanted to talk about why I felt guilty, and be listened to.
The other example relates to a midwife from my local hospital phoning me the day after Hugo died. In a cheerful voice, she asked how I was. I replied that Hugo had died the previous evening. It was evident she had not heard me, because continuing in that cheerful voice she said “Oh ok, I understand you are at home now, would you like a visit?” Even if Hugo had not died, the tone and content of the call was inappropriate. Hugo would have been 29 weeks at that stage and while the unit that cared for him is excellent, there is no way he would have been home by that stage. It seemed to be a failure of checking the notes properly.
These are all examples of health care staff using jargon, and impersonal medical terminology. I am sure (and hope) these staff did not intend to be impersonal or insensitive. I am sure (and hope) these staff simply failed to put themselves in these women’s shoes, to consider how they were feeling at such a sad and difficult time, and to offer empathy. In the example of the midwife who phoned me, she needed to have used a different tone to the one she would commonly use with the happy events of mums at home with their healthy babies.
Effective communication is something I am passionate about, for the benefit of patients – I have worked in the profession within the NHS for several years.
Thankfully, we do have positive examples of communication to talk about.
The woman who had a miscarriage gave this emotional account:
The ward matron ushered us into her office and apologised profusely. She gave me my tablet and then offered to answer honestly any questions we had. We went over everything again but this time we received compassionate and truthful answers. “Yes, it would hurt lots but you will be offered pain relief”. “You will need to stay the night”. “It will be hard but we will be here to help you get through it”.
In the digital age, most of us will take to Google to explore our diagnosis and prognosis to find out more. Of course, while the internet has many useful, trustworthy sites, there are many that are complete rubbish (this is true of every condition, not just baby loss).
As one mum said about her baby’s diagnosis
Probably the worst thing I did was google the condition when I got home.
I found the same about HELLP syndrome – it is so rare, there is little information about it, and much of what I read was terrifying – not helpful to my emotional recovery.
Patients need to be guided towards trustworthy sites. I was heartened to read that as the result of the involvement of a bereaved mum, one hospital’s website has “information specifically about fetal abnormalities as well as details of the team of people who will be looking after them. When they leave the hospital after diagnosis they are given the website address and the number of a counsellor so they can look at it when the shock has worn off”. The website also has some links to recommended forums.
Happily, I do have examples of better communication of my own to share: consultants (both obstetric and neonatal) listening to me, and patiently answering my questions without patronising being an important one. Vitally, I have found the majority willing to listen to and take on board my feedback, and seek to reflect on their practice and make changes were appropriate.
That is heartening progress, for the benefit of other women during the heartbreaking time of losing a precious baby.
Language matters, always.