Originally posted September 26, 2016 by Leigh Kendall
This post was written by Leigh Kendall, mum to Hugo who sadly died aged 35 days. The post was originally published on 26 September, 2016 on Leigh’s now defunct personal blog. You can get in touch with Leigh on Twitter at @LeighAKendall.
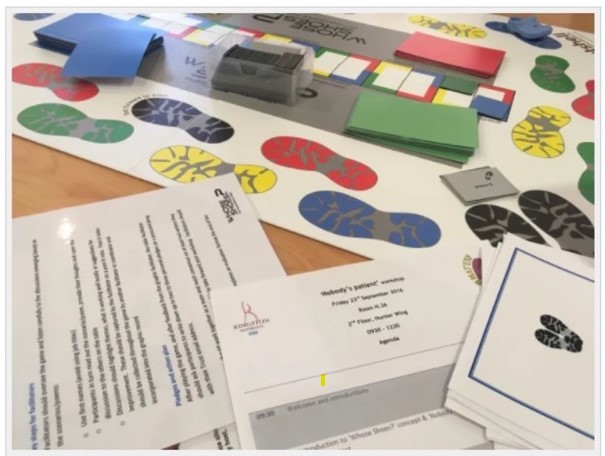
Nobody’s Patient workshop: St George’s Hospital – 26 Sep 2016
Friday September 23 was a special day, one I have been waiting on for a long time: the Nobody’s Patient workshop at St George’s Hospital.
The workshop is a key part of the Nobody’s Patient project and received funding from the Maternity Review Challenge Fund . The project evolved from the grassroots social media change platform #MatExp, and was inspired in part by my experiences with Hugo.
My beautiful Hugo
Bringing Nobody’s Patient to St George’s, where Hugo was born, lived and died is an achievement that means so much to me that it is hard to fully express using mere words.
The aim of the workshop was to get health care professionals involved in caring for families like mine to understand more about our experiences, and to make pledges to improve experiences for other families. I can’t change what happened to us, but through #HugosLegacy I wanted to help future families’ difficult experiences be a tiny bit easier.
The first workshop, in Kingston in early July 2016 was a huge success – everything was crossed for St George’s to emulate that. I was delighted to see so many people attending the workshop – all busy people prioritising the workshop over the million other things they have to do.
The workshop got underway: the room was full of buzz and ideas. Participants barely even stopped for refreshments so engrossed were they in the scenarios and discussion. All the scenarios are sourced from real people’s real experiences, which makes them very resonant, relevant, and often emotional – for both negative and positive reasons.
Communication was of course a topic that underpinned many of the discussions. Some of the key points from the table I was on include:
The suggestion that doctors could use drawings to help parents understand their baby’s condition. Parents are tired, stressed, and emotional – being in the NNU can feel like you need to gain a medical degree within days, and there is so much terminology to learn. Parents are constantly anxious, and their precious baby being attached to an array of beeping machines that are keeping their baby alive adds another level of terror. Visual aids such as drawings of anatomy can help parents understand – and in turn these drawings can help parents explain their baby’s condition and prognosis to family and friends, too. Doctors shouldn’t worry about their art skills – it’s about the concept rather than it being perfect! Anything that helps parents grasp complicated concepts is positive. There are some worries about notes and the formal medical record and governance, but the consensus was that drawings used as part of a conversation with parents are separate to the formal medical notes.
NNU mums often have difficulties receiving the necessary postnatal checks (whether or not they were ill during pregnancy, as I was). NNU mums’ priority is their baby, but their health matters too: they need to be as healthy as possible so they can be there for their baby, whatever the outcome. Our table discussed the concept of a ‘virtual ward’ where NNU mums could have their postnatal checks by identified professionals who crucially would have some training in the needs of NNU mums. Emotional and psychological needs of NNU parents are very often missed.
Dads and partners matter! Our table discussed how dads can be left out of the equation. There are times where they have been left alone after a traumatic birth, with blood everywhere and the in the delivery room looking like a scene from a horror film, their wife/partner and baby having been whisked away. The group talked about how in an emergency situation the room will be full of a range of professionals doing what needs to be done. Even if the procedure or equipment is routine, it may seem terrifying to the relative. Often after the emergency all the staff will leave the room with the patient, or go off to attend to other matters. Someone needs to remember to speak to the relative, debrief them, keep them updated, and give them information – not leave them standing panic-stricken.
I was heartened, especially after the disjointed nature of my own care, to see the dedication of professionals from various specialties keen to work together to give these mums and families the best possible experience and minimise additional stress.
Gill made this fab video of the awesome graphic facilitator Anna rounding up the feedback
In case you don’t have time to watch the whole video, some highlights amongst the many excellent pieces of feedback and pledges are:
A method of parents keeping an eye on their baby even when not physically present, eg FaceTime. This would have been so helpful to me when I was in intensive care in the hours before I was able to go and see Hugo, and for both Martin and I when we had to go and rest. Every neonatal parent needs to rest, and some parents need to go to work and/or care for other children too, so making use of technology would help parents feel able to be close to their baby at all times.
To see the mother and baby as one unit. The postnatal ward and NNU currently do not communicate well with each other; these links need to improve. In particular, the postnatal ward needs to better recognise the needs of NNU mums with things like expressing breast milk; food, emotional support, and being in the NNU with her baby as much as is possible.
Ideas to help parents understand and get involved with their baby’s care as much as possible, for example emoticons on the incubator to signify how the baby is doing.
The need for kindness, empathy, and understanding for any parent who is seriously ill during pregnancy, whose baby is cared for in an NNU, or whose baby dies at any stage during pregnancy.
Graphic by Anna Geyer, New Possibilities
After the conclusion of the workshop, we spent a lovely couple of hours in the First Touch garden, soaking up the glorious sunshine. This garden was designed by a NNU dad (whose lovely wife is also the charity’s director) and won a prize at Chelsea. The garden was moved to the front of the hospital for everyone to enjoy.
Flo, me, Catherine, and Gill in the First Touch garden
I would like to say a heartfelt THANK YOU to everyone who made this workshop a reality through organising it, and to everyone who attended. Martin and I cannot change what happened with me, and we cannot bring Hugo back. Helping other families through Hugo’s legacy helps us by knowing that Hugo can never be forgotten, and that his life has had purpose.
St George’s has been brilliant at listening to the feedback I have given them about the experiences of my own care and Hugo’s care, and has already implemented many improvements where necessary. I shall always be grateful to the hospital for saving my life, and for giving us 35 precious days with Hugo. The hospital and the staff who work there will always have a special place in my heart.
And, of course, Nobody’s Patient is about more than me, Martin, and Hugo. It is about ALL families who find themselves in a similar situation. We are working together to help prevent other families falling between the cracks of services, and avoid unnecessary additional stress and upset.
The St George’s and Kingston workshops are part of a pilot that we hope other hospitals nationally will take on board.
Because nobody should feel like they are nobody’s patient.
Leigh Kendall talks about the Nobody’s Patient project, Hugo’s Legacy, and #MatExp
Ever since Flo first phoned me, back in 2014, asking ‘if Whose Shoes would work in maternity services’, I have been impressed by her person-centred approach, her ability to challenge the status quo and push boundaries and to work WITH women and families. She lives and breathes her powerful ‘Wrong is wrong …’ mantra.
‘The Obs Pod’ will appeal to everyone who has an interest in maternity services. Everyone will be able to take something away from each episode, due to Flo’s wide-ranging experience, gentle reflective style and ground-breaking practice.
Gill Phillips, Creator of Whose Shoes? and co-founder, with Flo, of the #MatExp social movement
As a young Mum who was totally blown away by the inspirational obstetricians who delivered my baby nearly two years ago, I am excited to start following ‘The Obs Pod’. The first episode was fantastic; so interesting and captivating. I am sure the podcast will be hugely popular with pregnant women and maternity staff alike, along with so many other people who will find it fascinating to gain an insight into the thoughts and experiences of someone who shares the beauty and intimacy of pregnancy and birth as part of their working life.
Jenny Thirlwall, young Mum and member of #MatExp community, West Midlands
One of the things I have enjoyed the most over the last five years of #MatExp is the opportunity to get creative. From being ‘just’ an obstetrician, I have branched out and added: writer, poet, facilitator, film maker, speaker, campaigner to name just a few new skills.
Gill encouraged me to write a blog. I promised my husband it would be just the one, resulting in a nickname now from Gill ‘One blog Flo’. as I have lost count now of how many I have actually written after dipping my toe in the water.
I’ve enjoyed making Steller stories after a quick demo on a train journey, particularly our #MatExpAdvent series and my Nobody’s Patient monthly project reports. I have made videos, my contribution to our series for #MindNBody launch being one of my favourites, reading my poem ‘Reassured’. All this is alongside my day job and I find these creative outlets re-energise me, develop me and feedback into my day to day working in maternity care.
In December, I was lucky enough to meet Natalie Silverman @FertilityPoddy at RCOG women’s network meeting in Manchester. https://www.thefertilitypodcast.com/ She talked enthusiastically about podcasting. She made it sound both interesting and achievable. Something that wasn’t too challenging but that might reach a different audience. She was inspiring and willing to offer advice. I went home enthused.
I spent the next couple of months thinking and exploring, I decided I have things I would like to share. Adam Kay’s book ‘This is going to hurt’ has been a runaway success, but I want to voice a different perspective of the maternity world. One that would be accessible to women and staff alike. One that might ignite change and action as well as entertain. So, I have rolled up my sleeves, listened to a podcast series on making a podcast, taught myself the lingo, attempted the editing and technical bits and loved every minute.
So here goes, I am launching my next adventure: The Obs Pod. I hope you enjoy listening as much as I am enjoying making it!
Flo
Here are the episodes so far and new ones will automatically be added here. If you wish to access the programme notes Florence refers to each week, find the episode you are interested in on The Obs Pod (buzzsprout.com):
On Monday, to begin #ExpOfCare week, we had an insightful blog from Dr Sarah Winfield reflecting on her experience of taking part in the ‘Lithotomy Challenge’. And today, to end #ExpOfCare week, another #FabObs, Dr Florence Wilcock – the originator of the #LithotomyChallenge and co-founder of #MatExp – tells us all about Caesarean sections and what really happens…
Dr Florence Wilcock
As we come to the end of #ExpOfCare week, I would like to share a blog about Caesarean sections, to demystify the birth that mothers and partners may unexpectedly experience. I originally wrote this blog at the request of Milli Hill & the positive birth movement in October 2016 , subsequently this has been included as a contribution to Milli’s book ‘The Positive Birth Book’ published 16th March 2016.
Why do we need to talk about Caesarean sections?
Unfortunately, sometimes people can be prone to making value judgements about different types of birth. One of the most common examples is vaginal birth = good and Caesarean section = bad. The truth is that in the UK current statistics show 25% of women will give birth by Caesarean section, 10% planned so called ‘elective’ and 15% unplanned ‘emergency’. We can argue these rates back and forth; we can aspire to improve care and change these facts, but for the moment given that 1in 4 women will meet their baby in the operating theatre it is vital that we talk openly about this experience and how it can be a positive, emotional & fulfilling birth for each new family.
Even in an unexpected ‘emergency’ there are still choices to be made. Nice guidance on Caesarean section CG132 section 1.4.3.4 recommends 4 categories of urgency; only category 1, the most urgent suggests delivery within 30mins. Far more common is the ‘emergency’ caesarean category 2, delivery within 75mins of decision making. This gives a woman time to express contingency birth preferences and ensure that even if she did not plan a caesarean birth it remains a calm and positive start for her and her baby. Skin to skin in theatre, optimal cord clamping, birth partner announcing the sex of the baby, choice of music are all possible. I would love to say these are all standard in every hospital but unfortunately that wouldn’t yet be true, however the more women know and ask, the more these will become universally accepted. As I often say ‘Wrong is wrong even if everybody is doing it and right is right even if nobody is doing it’. I wish you all an interesting and positive month discussing Caesarean birth and would like thank Milli for inviting me to contribute & become part of it. If you want to know more about how I am working to try and improve maternity services do check out matexp.org.uk
Caesarean Section a theatre experience & Who is who in the operating theatre?
The majority of caesarean sections in the UK will be done under a spinal anaesthetic, that is numb from the nipples downwards. It’s a peculiar feeling as one can feel touch but not pain. It means that women will be awake and aware of people milling around them which can be daunting but it also means they are awake and ready to meet their new baby. Lying on the operating table we tilt women slightly to their left to keep the bump of the baby off the major blood vessels, this prevents dizziness from low blood pressure. If you lie on the operating table in the maternity theatres at my Trust you will look up and find butterflies & cherry blossom on the ceiling, something nice to focus on while you wait for your baby to arrive. I know this is unusual & we are lucky but there is nothing to stop you tucking your favourite picture or photo in your birthing bag so that you have something familiar and relaxing to look at.
It might seem odd that at the start everyone in the theatre will introduce themselves to one another. It isn’t that we have never met but its start of the World Health Organisation (WHO) safety checklist. There is a special checklist just for maternity theatres and it is routine to start by checking simple information such as the woman’s name and date of birth and move onto clinical issues and equipment and it is all aimed at making the experience as safe as possible. So, who are all these people around you and what are their roles, why are there so many people there?
Anaesthetist: At least one sometime two; these are doctors who will administer the anaesthetic ad monitor you closely during the surgery. They will be standing just by your head and often chat to you and reassure you as the operation progresses.
Operating Department Practitioner (ODP): at least one; their role is to assist the anaesthetist, getting & checking the required drugs, drips or equipment, the anaesthetist cannot work without one being present.
Obstetricians: at least two; one will be performing the Caesarean section (the surgeon) the other will be assisting (the assistant) e.g. cutting stiches, holding instruments.
Midwife: At least one; to support the woman and help her with her newborn baby when it arrives
Scrub nurse or midwife: At least one; To check, count all needles, stiches and instruments and to hand them to the surgeon when needed.
Midwifery assistant or runner: This person double checks the swab and instrument count with the scrub midwife or nurse and ‘runs’ to get any additional equipment required as they are not ‘scrubbed up’ so can go in & out of theatre to fetch things.
Paediatrician: asked to attend any ‘emergency’ situation or if there are known concerns about the baby.
So, you see in theatre there is a minimum of seven people caring for any woman all with specific tasks to perform, any complication may result in us calling in extra members of the team.
So back to the woman, she will be on the operating table with her birth partner by her side and the anaesthetist and ODP close at hand. She can often choose the music she would like her baby to be born to. The anaesthetist needs to monitor her heart with sticky labels but these can be put on her back and her gown left loose leaving her chest free and ready for skin to skin with her baby. A sterile drape will be placed over her bump and this is usually used to make a ‘screen’ so that the woman doesn’t see and surgery she doesn’t wish to see however usually we drop this when the baby is ready to be born.
Many hospitals are starting to explore options of optimal cord clamping (waiting to clamp the cord) and passing the baby straight to the mother if the baby is in good condition. These can be done but need to be thought through so as not to contaminate the sterile surgical area, and the surgeon needs to be confident no harm such as excessive bleeding from the womb is happening whilst these things occur. Surgical lights need to be on so the surgeon can see clearly and operate safely but I know one anaesthetist who works in a hospital where the rest of the theatre lights can be dimmed. The mum and new baby can be enjoying skin to skin whilst the rest of the operation proceeds. Weighing and checking babies can be also done at this time but also can be done later on.
Traditionally if we operate with women under a general anaesthetic (asleep) her birth partner has not been in in theatre as their role is to support the woman. Recently on several occasions I have challenged this so that a baby is welcomed to the world with at least one of its family present and awake rather than by a group of strangers caring for the unconscious mother. There are safety considerations to be talked through for this to be successful but it is possible. However, kind and caring staff are, they are no replacement for a birth partner whom the mother has chosen to support her in the intimacy of birth.
I hope I have given you a brief glimpse in to life in a maternity theatre. As an obstetrician, I am privileged to help bring many women and babies together for those special first moments. The emotions are always different for me: sometimes it is a couple I know very well and have bonded with over months or years, sometimes a woman I have only just met who has had to put her absolute trust in me immediately. The theatre atmosphere can range from almost party like jollity to quiet intimacy. Every birth is different; each birth is extremely special just as much as the births that happen in a less clinical environment and each birth will stay with that woman forever.
I was asked to do a talk to student midwives at Salford University in January on the topic of “Women’s Voices” in maternity care. As part of my presentation I included the voices of the midwives who work in maternity care, and a reminder that there are many other women for whom maternity care is their professional, as well as perhaps their personal, experience. “Women’s Voices” in maternity care should cover the midwives, obstetricians, health visitors, doulas who care for us, as well as the women giving birth.
So I decided to start a series of blog posts on “Women’s Voices in #MatExp” from the point of view of those working in maternity, and this is the sixth of those. This is Carolyn Johnston’s experience as an anaesthetist – thank you so much to Carolyn for agreeing to write for us. You can read the other blogs in the series here:
And yes, I will be doing a “Men’s Voices in #MatExp” series too. Because this campaign is about all voices.
Helen.x
*********************
Carolyn is a consultant anaesthetist in St George’s hospital in London.
Anaesthetics is usually the biggest department of doctors in most hospitals. We cover services including intensive care, operating theatres for all specialties and patient groups, resuscitation teams, pain management, and many other areas as well as maternity care. For those of us with a special interest and training in obstetrics are usually on the maternity unit for the day, but on other days we may be working on general (abdominal) surgery, transplant or any other kind of surgery, intensive care or whatever our other specialty interests may be.
In our unit, my day starts with a handover from the night team. The registrar (senior doctor in training) who has been on the maternity unit overnight tells us who has had anaesthetic input with pain relief (usually epidurals), any women who have been to the operating theatre and require ongoing care and highlighting anyone who may require extra vigilance during the coming day. This might be because of a pre-existing medical issue or developments in labour that may make care more complex. Because all anaesthetists have training that includes caring for people who are critically unwell and are part of resuscitation teams, we have the skills to help the maternity team care for lots of conditions that maternity teams may see very rarely (like heart disease) or those that are more common but might be serious if not treated early (like infection/ sepsis or heavy bleeding).
We also start the day by checking our equipment in the operating theatre and emergency medications. We must be ready to move at a moments notice if the situation arises, for urgent surgery or some other intervention, as we all know, maternity situations can change rapidly! These are scenarios we practice and refine until we can do them as safely as possible. Safety is a key part of anaesthetic practice, in our training we learn a lot about teamwork, safety theories such as ‘human factors’ and communication, and we check and practice a lot, so when we need to act quickly we can do so safely.
We will be involved in any planned (elective) caesarian sections during that day, in my hospital there are usually 2 or 3 cases planned per day. It must be so intimidating for a woman to come to the operating theatre; such a foreign environment and the idea of surgery whilst you are still awake must be so daunting. And then of course the nerves and excitement about finally meeting your baby! I see it as a big part of my job to help make that experience as positive as it can be, and help make women and their partners feel welcome, secure and hopefully even relax. Maybe even some skin-to-skin contact in the theatre.
Maternity work is very different from all other anaesthetic practice because unlike most of our other work, our patients are (usually) awake. This adds to the challenge: undertaking potentially difficult anaesthetic procedures, communicating with the theatre team, maintaining safety by monitoring and reacting to any changes in your patient’s condition but all whilst being mindful that the patient and her partner have holistic needs. Reacting to these needs and helping them to feel safe and secure is very important. There is always a balance to be struck with maintaining our best and usual practice for safety, and providing individualized holistic care. I think this is best achieved by talking and understanding each other’s perspectives. Perhaps we don’t do this enough.
We will, of course, respond to any requests for pain relief for epidurals, which is what most people think of when they think of anaesthetic involvement on delivery suite. It can sometimes be the case that women is distressed, distracted or even scared; so there is a real need for thoughtful communication and co-operation to help her and undertake the epidural safely. This balance of technical and people working skills is a common theme for us in obstetric anaesthetics.
I am lucky that our maternity team values co-operation and team working, and anaesthetists are an important part of that. It isn’t always the case that we are fully included in the team, and this can be a real source of frustration, because so many patients tell us our involvement is very helpful. We have a reputation (unfairly?) of being the epitome of intervention, so I guess we aren’t welcomed by some who hold strong views that birth should be natural. I have no desire to force my interventions on anyone- I would much rather put my feet up! Ultimately, I think the woman can make up her own mind, and as we pride ourselves on knowing the evidence, she should always get impartial advice about risks and benefits from an anaesthetist.
I’ve been trying to avoid the word ‘risk’- I know it’s becoming unpopular in maternity discussions. There is no avoiding it: anaesthetists deal in risk. We train and work in very high-risk areas including emergency surgery, trauma teams, heart surgery, intensive care and in those roles we’ve all seen someone die in front of us as we care for them. Anyone we look after is a patient, and rarely a client- it’s hard to switch this off when we come to maternity and so we often use terminology and even a more risk-based attitude that can clash with the modern ethos of maternity care.
I guess the solution to improving this is to talk more- to all our colleagues in maternity care and to our patients- we all have the same aims and aspirations to provide the best care for healthy happy mums, dads and babies. We also have a reputation for loving coffee, so my suggestion is to grab an anaesthetist on your precious coffee break and ask each other: “why are we all here and what skills do we bring to make that happen?”
This post is from Michelle Quashie, and originally appeared on her blog site Strong Since Birth. Our thanks to Michelle for agreeing for it to be reposted here.
The day had finally arrived! After contributing to #MatExp and interacting with many conversations surrounding ‘WhoseShoes’ throughout the year, I was finally going to experience the magic in real life.
Laura, the chair of our MSLC has written a fantastic post that captures the excitement of the day perfectly, you can read it here: When WhoseShoes Came To The PRUH
I was not disappointed, the day was everything I had dreamed of, but for me it was so much more.
I was asked to open the event by sharing my Maternity Experience. I have spoke at several maternity training events in the past but my audience has always been Midwives. I was aware that this was a multi discipline training event and it was to be the first time I would share my story in such detail with Obstetricians and everyone else involved in Maternity. The thought made me feel anxious but I knew how important this opportunity was.
I had planned to stay in control and not let the emotions attached to my experience be displayed in the form of tears. It was so important to me to remain composed and in control.
My heart pounded through the showing of the MatExp film, this film moves me every time. It is so powerful and very thought provoking. Sadly I can resonate with many of the situations displayed in the film. I knew I was about to be discussing some of those memories any minute with all those surrounding me.
My name was called and I made my way to the front with my heart pounding. I decided to be honest and share how I was feeling with the room.
‘Please bare with me, I am feeling very nervous. I’m sure once I start talking I will warm up and I will be fine!’
Automatically I felt more relaxed and felt more able to share my story without the anxiety overruling my thoughts.
It’s amazing how every time I share my experience it comes out slightly different, or I find myself saying things that I hadn’t thought of before? I had missed a couple of important bits out but neither the less I was very happy with the way I had presented and gauging by the feeling of emotion in the room I had touched the hearts of nearly everyone around me. For the first time I was able to keep my tears to myself even though I had noted that tears were shed by many in response. The room fell silent but the atmosphere spoke volumes.
I wasn’t aware of the tweets that were being circulated on social media but looking at them them later along with the emails I had received It confirmed that my talk was a positive part of the day.
“Also a massive well done to Michelle for her heartfelt and emotional story, I could see it touched many people as there were certainly a few tears in the room. That took huge courage to stand there in front of so many people and share such a personal experience and to tell it so well. Huge WELL DONE Michelle.”
We began to play the the game and interesting discussions were had in response to the thought provoking questions that are key to the WhoseShoes success.
Some of the discussions that stick in my mind were:
A woman wanted a home birth but her husband wasn’t convinced. We had discussed that there wasn’t enough support or information given during antenatal care to ensure that the couple felt safe,supported and empowered to fulfil the woman’s birth choice.
Consultant Obstetricians are normally addressed by other members of their team using their title i.e., Sir, Mr, Mrs or Miss as a mark of respect. I may be wrong but it feels hierarchical, unlike the power slogan and barrier breaker behind WhoseShoes and #MatExp ‘No Hierarchy, just ordinary people’.
It was also discussed that consultants were on site until 9 pm, after that they are on call for emergency situations only. Now I understand why during my appointment to discuss my VBAC, the registrar said ‘ I mean, we don’t know when you will go into labour or who will be on duty should you rupture’. I now understand that my birth choices were influenced by staffing levels at the hospital.
Other key themes were Empathy, Language, supporting and facilitating informed decision making and just how important it was for everyone to be cared for individually based on their individual situation and needs.
Midwives are able to have time to build a relationship with women whereas doctors are often called for the emergency situation and do their best to resolve the medical issue as it arises. This can sometimes make it hard for them to be able to connect with the woman that they are caring for and are not always able to fully appreciate the long lasting effects the experience can have on a woman.
The day was coming to an end and Anna gave us fabulous evaluation of our morning using the comments that came from the discussion at each table. It was fabulous to visualise the discussion using the graphic that Anna had been working on through out the morning.
We each made an individual pledges. Here is my pledge:
“To provide a platform for women to share their Maternity experience. I would like to ensure that women’s voices are heard as part of training and development.”
I am currently planning a conference called ‘Women’s Voices’. More details will be available soon.
As the morning came to an end and people were leaving someone tapped me on my shoulder. I turned round and my tummy flipped. The face before me took me straight to a place of feeling vulnerable, feeling panicky.
‘Michelle it was me wasn’t it?’
Stood before me was the registrar that I had my consultation for my vba2c with. Unbeknown to my self and the organisers we had shared the morning. I had shared an experience that changed my life but had also been a time that left me feeling scared, vulnerable, isolated and questioning my mental health. The person that was responsible for those feelings was standing here in front of me, for a moment the feelings came flooding back, I battled to keep them contained.
She apologised for the way she had cared for me. She admitted that she had been wrong and has since ensured that she was fully aware of her professional guidance. She was now fully supportive of women’s choice regarding their birth and ensured me that since having to write a statement in response to my complaint, she is fully aware of the impact of the care she provides a woman.
She actually thanked me for highlighting the error of her ways promising me it had changed her attitudes. I could see that she was overwhelmed with emotion and had spoke to me honestly. She asked if she could hug me and we both held each other for comfort.
I told her that I admired her for taking the time to come a talk to me and for apologising. I also explained that I was aware that she was not entirely to blame for the care I had received and I now understood that her response to me wanting a vaginal birth after two caesareans was due to the cultural belief of the trust she worked in.
It was clear that my birth wishes would not be supported and neither would anyone wanting to support me at that time. I know this because many attempts were made to provide me with the support I needed and no one stepped out of their comfort zone to provide me with the support I needed with regards me birth choices. As a result I had no choice but to transfer my care.
She empathised and promised me that as a result of my experience things were changing.
We said our goodbyes and I was trying very hard to contain my emotion that the meeting had evoked.
A consultant midwife that has walked by my side through this maternity experience and others and who has been a pillar of support to me came to see me. ‘Are you OK Michelle?’
The flood gates open and I broke down. I couldn’t talk at that moment. I was just overwhelmed with emotion. I couldn’t make sense of it at the time but now I think I can.
That meeting with the registrar brought some closure. I admire her ability to acknowledge the error of her ways.
The meeting took me back and reminded me of the scared women I once was sitting in her office, trying to persuade her that I could give birth, pleading with them to allow me. Feeling so horrible when it was highlighted that I had never given birth and they wasn’t sure if I could. I was subjected to a number of negative comments that effected my mental well being and left me questioning my sanity. Comments that left my family feeling unable to support my decisions in fear of my safety. it was a meeting that left me feeling isolated.
Here I sat after coming full circle with the same women but this time I was a different woman. I am a now a woman who has had the most amazing journey and have achieved some incredible things;
I gave birth, not only did I give birth but I bloody rocked that labour ward!
I came back and I told the story, I sang it from the rooftops!
I learnt to believe in me and my abilities.
I joined their MSLC and contributed to so many fantastic improvements within the Maternity service.
I have spoke at training events within maternity with an aim to improve maternity care for women.
I have written and had my views published here and in The Practising Midwife .
I have contributed to #MatExp campaign and connected with some fantastic people as a result.
I have met, received support and been inspired by many fantastic people. too many to mention.
The realisation that my shoes have climbed a mountain has happened!
I received the following email from a Consultant Obstetrician following the Whose Shoes event. It confirmed that this journey has been worth every little step:
“Dear Michelle,
I just wanted to reiterate how touched I was by your story and how impressed I was by the way you delivered it. You will be responsible for improving the practise of every obstetrician in that room today which in the end will improve the care of tens of thousands of women.
I have great pleasure in introducing a guest blog from Kirsty Sharrock, a.k.a. SouthwarkBelle. Kirsty is mum to two girls and lives in London. Her other day job involves biological samples, powerful lasers and badly fitting lab coats. When her first child was born in 2009 she became fascinated, and often infuriated, by the amount of misleading information aimed at new parents. Her response was the SouthwarkBelle blog where she tries to make sense of some of the dubious science or at least have a good rant about it.
Thank you so much to Kirsty for writing for us on the topic of Induction of Labour.
Kirsty Sharrock – SouthwarkBelle
It’s a well known fact of modern childbirth: Inducing labour sets off a chain of other interventions which often result in an emergency caesarean.
But is this actually true?
Would you be surprised if I said it’s not? I certainly was. The idea goes against so much that I had heard from other women and from midwives, my antenatal teacher and of course the internet.
When I went overdue with my first baby I dreaded being induced. I’d heard nothing but horror stories saying it was entirely awful and unnecessary, it would almost certainly make the birth more painful and complicated and would probably set off a “cascade of interventions” leading, with grim inevitability, to the one thing I was most afraid off – an emergency Caesarean. It would also completely scupper my plans for a natural birth in a midwife led unit. But at the same time I was MASSIVE, it was August, and hot, I was desperate to meet my baby and had had quite enough of being pregnant. So I agreed to book an induction, then did everything I could think of to make that booking unnecessary. In the event I got my wish, sort of.
41 weeks and feeling massive
So was I right to fear the induction?
It seems the answer to that is no.
A 2014 study showed that being induced doesn’t increase the likelihood of having a caesarean. In fact women who were induced at term or when overdue were 12% LESS likely to have a C section than those who hung on for nature to do her thing. Their babies were also less likely to be stillborn or admitted to the NICU.
But can we believe this study?
We often see piles of scientific “evidence” that contradict each other. One minute coffee causes cancer the next it cures it etc. etc. so how reliable is this publication, given that it goes so strongly against the generally accepted view?
In this case the authors of the paper didn’t set up their own experiment or trial. Instead they did what is known as a meta-analysis. This is important because a meta-analysis is far more reliable than most of the scientific studies that make it into the media. The authors took the data from 157 different trials and did some serious number crunching. Looking not just at the results of those trials but at their weaknesses too. For example, many of the individual trials were pretty small, meaning their results are less reliable than bigger studies. Others were quite old or asked slightly different questions to the rest. But this variation is the whole point of a meta-analysis. By putting it all together it’s possible to overcome many of the errors and biases that inevitably influence the results of individual studies and to find a more reliable consensus.
We rarely get perfect answers in anything associated with biology. For obvious ethical and practical reasons we can’t do loads of enormous, randomly controlled trials to answer questions about human childbirth. So a meta-analysis, although still imperfect, is about as good as it gets.
But how can it be true when it contradicts so many people’s experiences?
This is the really tricky part. These results fly in the face of something many of us have learned to be true: In the experience of many women, midwives, etc. inductions tend to end in C sections. As yet I don’t know of any scientific studies to explain this difference, but if we step away from numbers and statistics for a moment, there are a few, very human, possibilities:
Relying on personal experiences is tricky. We’re all inclined to notice and trust things that confirm our existing beliefs. That’s just human nature, and it happens to everyone (I’ve known a few, usually logical, scientists get carried away over flimsy results that fit their current theory). In this case perhaps midwives and doctors who expect inductions to end in c sections are just a little more likely to remember the ones that do. Those births may also stick in the mind more than the less eventful, straight forward ones.
A similar thing can also happen with women’s own experiences. Even with everything seemingly perfect, births don’t always go to plan. Difficult births happen and sometimes they happen after an induction. If a woman has heard many times that inductions cause c sections, then it’s only natural to assume the induction was to blame if she does end up in theatre. Maybe that was the cause, but there is no way to be completely sure that the same things wouldn’t have happened with a spontaneous labour.
There is also the risk of self-fulfilling prophecies. It’s possible that some women are ending up in theatre just a little earlier than they need to because they, or those caring for them, suspected it was inevitable. Perhaps most importantly, there is the issue of fear. It is thought that fear can be a big cause of problems in childbirth. If a women is induced, and terrified of the procedure and what she’s been told it will lead to, then it could be the fear itself which causes the problems.
So should every woman be induced at full term?
What this study doesn’t do is prove that all women should be induced the second they hit 40 weeks.
There are many reasons why a woman may decide to delay or refuse an induction. I went into labour naturally but still ended up having some of the interventions that can be used in an induction and I found them pretty unpleasant. Every woman and every birth is different and each comes with a unique set of considerations. Meta-analysis and big data sets give us a clearer and more objective view of the big picture but they can’t say what is right or wrong for any individual mother. That choice must be hers and to make it women need good, evidence based information and often help from skilled, knowledgeable, health care professionals.
This paper also doesn’t give us is a very clear picture of just how likely it is that an individual induction will prevent a c section, still birth or NICU admission. What I hope we will see in the future is more user friendly data. Every women will have their own tipping point for where the numbers add up to choosing induction.
Looking pretty rough after a labour that started naturally, but still ended in an emergency caesarean
So what now?
Like many pregnant women I was taught to fear induction of labour and the cascade of interventions it would cause. Now it seems that fear was based on a myth. So it’s important that the evidence, challenging though it may feel, gets out to pregnant women and to those giving them advice. Unnecessary fear in childbirth is potentially harmful and certainly unfair. All the more so for those women who feel they have little choice but to be induced for urgent medical reasons.
This study also has implication beyond individual decisions. There is often a binary division of births. On one side the “low risk”, “normal” births that can be handled entirely by midwives and on the other “high risk” births, which are, effectively, everything else. Being induced can push an otherwise low risk woman over that line.
In the hospital where I gave birth this made a big difference. The Midwife led unit didn’t just have lower all round intervention rates, it also housed built in birthing pools and lovely en-suite rooms where mum, dad and baby could recover together after the birth. If I’d been induced I wouldn’t have been allowed on this unit. So, in choosing weather to be induced or not, I wasn’t just weighing up the risks of induction v continued pregnancy. I was also deciding if I should risk higher intervention rates, sacrifice the more welcoming facilities and deny my husband the opportunity to share the first precious hours of his child’s life. Now we have strong evidence that induction can reduce C section rates and in some cases save lives, should it really be the determining factor in where some women can give birth? Or in the standard of care they receive?
For me, spontaneous labour didn’t prevent an emergency C section. Perhaps I’d have stayed out of surgery if I had been induced? I doubt it, although I’ll never know for sure. But I can be glad that when other new mums are overdue, concerned about their baby’s health or just hot, heavy and sick of being pregnant, the myth of induction-cascade-caesarean section will be one less thing to fear.
There has been much discussion recently about safety within maternity services including a discussion on #MatExp Facebook group. A particular issue that bothers me is the idea that safety and experience might be two separate and mutually exclusive issues and it is this thought that drives me to write today.
Safety is paramount. The purpose of maternity services is to provide safe care through the journey of pregnancy and early newborn life. Every appointment in the NICE pathway is designed to screen for potential problems and ensure they are managed effectively. Every healthcare worker know this is the aim. The 20 week ‘anomaly’ scan might be considered the time to discover the sex of your baby if you wish and to get some photos but the medical purpose is to ensure the baby is growing well, with no abnormalities and to check where the placenta is localised to exclude placenta praevia (low lying placenta) which can cause life threatening bleeding.
But there is more to pregnancy and becoming a parent than safety isn’t there? I am currently reading Atul Gawande ‘Being Mortal’ where he eloquently demonstrates that keeping elderly people ‘safe’ is not enough, there is more to life and living than safety alone. He describes a number of times when giving elderly people purpose such as a plant or animal to look after or more freedom to live the way they wish despite disability it makes a significant difference to their wellbeing. Sometimes this path may deemed ‘less safe’ but for that individual may make all the difference. This comes back to choice. Safety & choice can be tricky ones to combine successfully.
This does not mean I am belittling safety. As a consultant obstetrician it falls to me to talk to couples when the worst has happened and their baby has died. I also care for women who have had unexpectedly life threatening complications. I know I am with them during probably some of the darkest hours they will ever experience. I cannot pretend to understand how they feel but I do know I have been part of those intimate moments of grief and with some families that has followed through into supporting them sometimes for years. As a hospital we have a robust process of incident reporting and the feedback from a Serious Incident investigation (SI) again will sometimes fall to me. In some cases there is nothing that we think could have been done differently in some cases I have to sit and tell an anguished couple that we have failed them and that maybe things could have been different. It is a devastating thing to do, there is absolutely nothing that can be said that will make the situation better. It feels as if you have personally taken their existing despair and dragged them into an even more unthinkable place and the only thing you can say is ‘sorry’ which feel hopelessly inadequate and trite for such a situation.
So if I could guarantee safety I would in a flash but it is not that simple. Maternity care is delivered by people and unfortunately to err is human. We cannot design a system free of risk because however hard we try the variable of human error gets in the way. We can introduce systems that help minimise the impact of these errors but we can’t eliminate them. My favourite analogy for risk management is James Reason’s model of Swiss cheese. The event only happens when the holes in the ‘cheese’ line up the rest of the time the barriers put in place prevent the error. An example in maternity care might be the introduction of what we call ‘fresh eyes’. A midwife looking after a woman on electronic fetal heart monitoring might misinterpret this or not see the subtle changes over time if she has it in front of her constantly. ‘Fresh eyes’ means another midwife or obstetrician comes and looks at the trace on an hourly basis. This means if unusually the first midwife has made an error there is a system that means it is more likely to be corrected.
The concept of a ‘No Blame’ culture is another example designed to minimise human error. The idea that if one sees or makes an error one should report it without fear so that learning can be gained from it. It may be the learning will be the need for some individual training but equally it might be something totally different. If staff are fearful of consequences then under reporting might be the result and safety gaps may not be identified. Encouraging openness about mistakes and errors is vital but difficult. In maternity it isn’t as if we can just operate our way out of this problem .We know the huge rise in Caesareans sections in the last 30 years has not improved the outcomes for babies but has instead cause maternal health problems. So in maternity as other medical specialties we have to constantly refresh and re-invent what we are doing to try and improve safety. As obstetricians we tread a difficult path trying constantly to call correctly just the right amount of intervention at just the right time.
So where does experience fit in I hear you ask? There is abundant published evidence of positive association of patient experience with clinical safety and effectiveness, in other words if your patients (or I prefer users) are having positive experiences then you are running a safer service. It’s hardly surprising if we communicate and explain things to women and their families that we will be more likely to communicate effectively to other members of the multidisciplinary team. If we are open and honest then woman can challenge assumptions and make sure we haven’t missed something critical, a woman knows her own history inside out whereas we might omit a key point. To me one of the most shocking things that was said at our ‘Whose shoes’ #MatExp workshop last year was that women can feel intimidated and unable to ask questions. Trust and understanding between health professionals and those we care for are vital. We cannot possibly hope to improve safety in isolation, experience has to improve too.
There are two specific elements of #MatExp of which I think epitomise the safety -experience overlap. The first is an on-going ever growing constructive conversation between women, families, obstetricians, midwives, health visitors, paediatricians, families and anyone involved in maternity services. Only by tackling the difficult conversations without hierarchy in an equal and respectful way can we improve maternity care. Listening and talking to one another is critical not only as we work with women but in dissolving those barriers and difficulties that sometime exist between different professionals. Flattening of hierarchy, team work and the ability of anyone to challenge is a well-recognised component of a safety culture. We are doing this both locally using the workshops and board game and more broadly via social media and the website.
The second element of #MatExp is that personal sense of responsibility to take action. Own what you are doing and why you are doing it. ‘Wrong is wrong even if everyone is doing it’ that doesn’t mean leave it to someone else. It means that health professionals and women can take action and influence maternity experience up and down the country and through that impact on and improve the safety of maternity care. So in final answer to my question I do not think it is a choice safety or experience I believe the two are fundamentally intertwined. So what will you do to improve #MatExp?
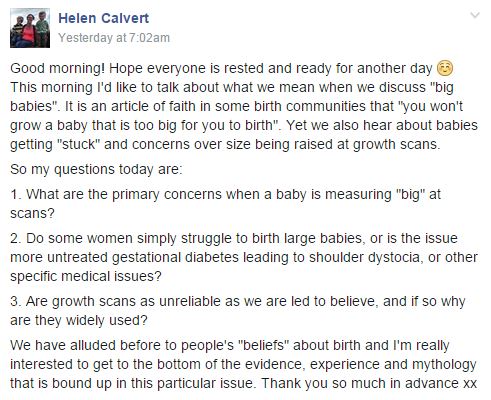
A while ago on a Facebook birth forum I saw the phrase “you won’t grow a baby too big for you to birth”. It was a familiar phrase as it was something I would hear regularly on the homebirth e-group I was a member of back in 2010 when I was pregnant with my first. Back then I accepted it as the truth, but having been involved in #MatExp for nearly a year I have learned that few things to do with birth are that simple. So I asked the question on the #MatExp Facebook group:
What followed was a fascinating discussion. Information was shared from lots of different quarters, and evidence was linked to. Experienced birth practitioners shared their views and a few themes started to appear. All along I knew I was intending to write up the discussion as a blog post so I was trying to keep up with the information and understand what was being said. As I opened up links to studies, trials, journal articles and so on my heart sank as I am not the best at analysing that kind of thing and it seemed at first glance that the evidence shared was somewhat contradictory. So I was concerned that I would end up inadvertently talking rubbish in this post.
And then I realised that this is exactly the problem. I am a woman of childbearing age who has had an education to degree level, English is my first language and I discuss birth and maternity pretty much every day. When we talk about informed choice we mean sharing all of the evidence plus the benefit of experience with pregnant women and their families, so that they can go through it and make their own decisions. Yet if I were writing this today as a woman who had been told she was likely to have a “big” baby I would be confused. And a little scared.
So it’s a good job I didn’t know any of this when I confidently went on to give birth to my 8lbs 13oz son on all fours on our bathroom floor.
Let’s pretend for a moment that I am in my third trimester and have been told by my midwife that she suspects baby is going to be a big ‘un. Probably a bouncing 9lbs tot. Before I go down the route of “doing” anything about that, or amending my birth plans, I have asked the #MatExp group for some information. What have I discovered?
Well, firstly we need to know a little bit more about this fictitious me. Do I have gestational diabetes? Am I classed as overweight? No? Okay then, we can stick with our issue being only the predicted size of my baby and keep questions of GD and BMI for another day if we may. Similarly, we will assume that I am physically able. So why are people sucking their teeth and looking concerned that baby might be of a generous size?
This is where we come to shoulder dystocia. “Shoulder dystocia is when the baby’s head has been born but one of the shoulders becomes stuck behind the mother’s pubic bone, delaying the birth of the baby’s body. If this happens, extra help is usually needed to release the baby’s shoulder. In the majority of cases, the baby will be born promptly and safely.” (From https://www.rcog.org.uk/en/patients/patient-leaflets/shoulder-dystocia/)
In the majority of cases, the baby will be born promptly and safely? So what’s all the fuss about then? Well let’s look at this passage from the abstract of this article:
“Shoulder dystocia remains an unpredictable obstetric emergency, striking fear in the hearts of obstetricians both novice and experienced. While outcomes that lead to permanent injury are rare, almost all obstetricians with enough years of practice have participated in a birth with a severe shoulder dystocia and are at least aware of cases that have resulted in significant neurologic injury or even neonatal death. This is despite many years of research trying to understand the risk factors associated with it, all in an attempt primarily to characterize when the risk is high enough to avoid vaginal delivery altogether and prevent a shoulder dystocia, whose attendant morbidities are estimated to be at a rate as high as 16–48%. The study of shoulder dystocia remains challenging due to its generally retrospective nature, as well as dependence on proper identification and documentation. As a result, the prediction of shoulder dystocia remains elusive, and the cost of trying to prevent one by performing a cesarean delivery remains high. While ultimately it is the injury that is the key concern, rather than the shoulder dystocia itself, it is in the presence of an identified shoulder dystocia that occurrence of injury is most common.
The majority of shoulder dystocia cases occur without major risk factors. Moreover, even the best antenatal predictors have a low positive predictive value. Shoulder dystocia therefore cannot be reliably predicted, and the only preventative measure is cesarean delivery.”
Ah, okay. So whilst MOST cases are not a problem, when there is a problem it can be very serious. And most experienced obstetricians will have seen this happen, inevitably influencing their perception of the risks involved. The teeth sucking is a bit more understandable now.
Apparently if I have a small pelvis it is more likely that baby will get his shoulders stuck. How do you know if you have a small pelvis? Small compared to what or whom? I have no idea but it appears to be a consideration. One birth professional observed that “to me that ‘big’ is subjective in a lot of cases. A 7lb baby could be big to one woman whereas a 10lb baby could be average to another. There needs to be far more than just the picture provided by a (often inaccurate) scan. Woman’s own birthweight for example, her stature etc.” It was mentioned that pelvimetry used to be widely used but has been abandoned in favour of scans, due to a Cochrane review that found these measurements did more harm than good.
There is a higher likelihood of shoulder dystocia in bigger babies, that much is undisputed. Yet the language used when discussing this risk makes a big difference to how a pregnant woman might view the risk. Contrasted with the passage above is this from Evidence-Based Birth:
I suspect as with so many birth choices, women are likely to get the reassuring language from midwives who have confidently dealt with many instances of stuck shoulders, and more wary language from obstetricians who have seen first hand what can go tragically wrong.
So in summary shoulder dystocia is more likely in bigger babies but on the whole it can’t be predicted and can usually be dealt with. It turns out that there are arbitrary cut offs for recommending Caesarean to prevent SD – 5kg in a non-diabetic woman. That means nothing to me but a quick Google tells me that is an 11lbs baby. My hypothetical nine pounder doesn’t warrant an automatic recommendation for a c-section then. So far so good.
But what position is my baby in? This is an important factor. I would argue that all pregnant women should be aware of foetal positioning and how to optimise it, but in this case it is particularly important as a malpositioned big baby could cause trouble. Let’s assume though that I have been on spinningbabies.com, haven’t been reclining on the sofa, have been doing headstands for nine months or whatever it is that is recommended. Baby is now head down and engaged and we’re ready for the off.
At this point it’s good to know that there is no evidence to suggest that it hurts more to give birth to a big baby. I cannot comment as my firstborn is the only child I have birthed vaginally so have nothing to compare it to. But the midwives on the group have been reassuring that being predicted a “big” baby does not mean increased pain in labour. Good stuff.
What I haven’t done (but what might have been recommended to me) – I have not had a growth scan. It appears that growth scans should be used to identify small babies (a discussion for another day no doubt) but not big ones. One group member commented “Ultrasound scans become increasingly unreliable the further along in pregnancy they are performed. Weight is an ESTIMATION can be up to 25% out either way. They base it on the abdominal circumference, head circumference & femur length – try doing it with yourself & see how accurate it is!”
A birth professional went on to say “Growth scans are pretty hopeless in the third trimester – the only thing that is useful is a regular plotting of growth to try to identify a sudden growth spurt that could indicate a problem. A one off growth scan late on in pregnancy basically just leads to unhelpful fears on all sides.”
Which begs the question, how do we identify the potential 11lbs babies who “require” a c-section birth?
So I haven’t allowed anyone to worry me further with a most likely inaccurate scan reading. We think baby is going to be big but not so big that I am going to be encouraged to have an elective c-section, so I’m happy to go ahead with my vaginal birth.
This is where we come to the issue that dominated the discussion. The position that women labour in can make a HUGE difference to the outcome when they are birthing a large baby. Labouring on their back is most likely to be unhelpful. Labouring on all fours is most likely to enable them to birth without intervention. Certainly my experience – I could not bear to be in any position other than kneeling up for my entire labour, simply could not bear it. Lying down was absolutely out of the question.
One group member had a wealth of information to contribute and commented “There’s plenty of evidence to support programs like birth ball use, not just gentle bouncing but using as a structured exercise plus also designing maternity units/rooms to encourage movement and position changes and upright movement.”
A midwife explained “I worked with a lovely obstetrician a few years ago (I have worked with many wonderful obstetricians). She was leading the skills and drills component for obstetric emergencies of the yearly mandatory training. We were practicing what to do in the case of a shoulder dystocia with a mannequin. She looked at me and said, of course we all know that if we do this (turning the model over in to what would be an all fours position) we wouldn’t have to be doing this at all.”
And one of our obstetricians added “in terms of labour progression, size is not nearly so important as baby’s positioning and flexion.”
The impact of pain relief was also mentioned: “Of course this is impacted by maternal position too, often compounded by an epidural that softens the pelvic floor muscles reducing the baby’s ability to rotate on the pelvic floor.”
Let’s recap. My midwife has said that it is her experienced opinion that I am going to have a big baby. I have declined a growth scan but we are both confident that baby won’t be topping 11lbs. So we’re going for a vaginal birth, and have done everything we can to ensure baby is in a good position. I am then being encouraged to be active in labour, labour on all fours and so on. There is no reason to believe that I will experience more pain due to baby’s size. There is an elevated risk of shoulder dystocia but my birth team are trained to deal with that. Hmm, okay, on reflection I would make the same choice I made back in 2011 when I hadn’t had this conversation. Home waterbirth with experienced midwives please! Especially, for me as an individual, “big” babies are normal – I was 9lbs 11oz at birth myself.
Does the above sound like the experience most women have when a big baby is predicted? Let’s ask some real life women shall we? Here I am indebted to the fabulous women on my other Facebook group who have shared their stories with me.
“I was told I would have a big baby. The midwife measured me way off the chart at 36 or 38 weeks can’t remember which. Went for growth scan. Again measured me pretty big. Appointment with consultant, he measured me big. Straight aways did a growth scan. I was then booked in for an induction the following week. Was in from the 25th and had him on 29th (due on 5th July) he was only 8lb 2oz.” What was the reason for the induction? “Not sure. They said as it was my first I probably would go over so as he was measuring big now it could be more of an issue in 3 or 4 weeks.”
“My 1st baby was 9lb 14oz and got stuck with shoulder dystocia and born with the ventouse.” And what positions were you labouring in with baby no. 1? Were you on all fours at all? “No! I believe position/ventouse were what caused her to be stuck! I was dehydrated so they made me stay in the bed on my back to be monitored!”
“I was told my little boy was a big baby and I had to have a growth scan. I was then induced a week early due to his size. He weighed 8lb 15oz and I had a 4th degree tear and had to be rushed to theatre.”What did they say were the risks with him being big? Did they explain why they wanted to induce you? “The explanation for me being induced was if I was left and went over I would have had a tough time, but looking back now I wish I had opted out of being induced as I blame that for the complications.”
“I was measuring big for dates at my midwife appointments from about 24 weeks. I was eventually sent for a scan to rule out polyhydraminos at about 32 weeks. The scan results were ok and showed that my baby’s measurements were on the 95th centile. I was then changed to higher risk consultant led care. They told me it was due to the baby’s size and the increased need for intervention during delivery, e.g. forceps, etc. My baby was predicted to be 9lb 9oz maximum and she was actually 10lb 6oz. I was in slow labour for 6 days. I had to have an oxytocin drip to get me from 7cm but I couldn’t get passed 8cm as her big shoulders meant her head wouldn’t press down on my cervix! As a result of being on the drip, I wasn’t able to get in different positions in labour and was mainly confined to the bed. I then had an emergency c-section due to failure to progress.” How did all the talk of having a “big” baby affect how confident you felt in being able to give birth? “To be honest, it did affect how confident I felt giving birth. I was then very nervous at the prospect of tearing or that I’d have difficulties during the birth and would need forceps, etc. I was very worried that something would go wrong. To be honest, I felt very relieved when the consultant said I needed a c-section.”
I commented that I wondered whether that was the reason the mum above struggled to dilate. Rather than failure to progress perhaps her caregivers should be have been labelled with “failure to encourage”.
There was one rather different story, although the mum in question was surprised by how her consultant’s advice varied from what others were experiencing: “Was told based on my daughter being 10lb that my little boy would be big. The midwife referred me to a consultant as my fundal height was bigger than even my little girl was! Tested me for GD which I didn’t have. Consultant said he was going to do absolutely nothing about it which varied massively from my peers at nearby hospitals who were being induced early. He said inducing a large baby is dangerous as they’re more likely to get stuck and if I got my little girl out this one would be fine! Bit worried but I trusted him.”
And what of those women who had not been told to expect a big baby?
“I had a 9lb 4oz baby but wasn’t expecting him to be ‘big’ I had a tiny bump and was told he was only going to be about 7lb. I had him naturally with no complications at all. A few stitches externally but that was all.”
“My 2nd baby was 9lbs 6oz and no one knew he would be that big as my first was 7lb 11oz. Labour was very quick and vaginally delivered with 1 stitch.”
“If 9lb2oz is classed as a big baby then mine was! He was 13 days over so probably wouldn’t have been so big if I’d gone on time. Nobody told me he was going to be big at any of the extra monitoring appts I had the week before he arrived all on his own, no help, drugs or hospital. I did tear slightly but midwife was happy for me not to go to hospital if I didn’t want to.”
“I wasn’t told I was going to have a big baby, I was tested for diabetes at one point because my bump had grown quite quickly but I didn’t have it. My little boy weighed 9lb 15oz, I was in labour for 6 and a half hours and didn’t have any complications. I had a few stitches afterwards but nothing major.”
What can we say in conclusion? When a baby is identified as potentially being “big” are all families given the information that we have discussed here? Do all birth professionals agree with the general thrust of this post or have some important points been missed or misrepresented? And if I have got it all wrong what does that say for the idea of “informed choice”? Because this is my best understanding of the issues following a detailed discussion with experienced birth professionals. There are plenty of other birth stories from the mums on my group which make it clear that women are routinely being encouraged down the route of induction without fully understanding why, only that baby is going to be “big” and that is some kind of a problem. And so many of these stories end in instrumental deliveries, emergency c-sections and, at worst, traumatic births. Would it not be preferable for women to have the issues fully explained to them and to be encouraged to have an active birth where, in all likelihood, they will be capable of giving birth to their child?
I am just glad that my “big” baby is here, safe and well, and now in his second week at primary school. Decisions always seem simple in hindsight.
Some of the links that were shared as part of the discussion not already linked to above: