I am an avid follower of #TheObsPod and I was excited when #FabObs Florence Wilcock, who tweets as @FWmaternity, said she was producing an episode around disability in pregnancy. You can listen to it here: Episode 56: The Obs Pod – Maternity Experience (matexp.org.uk)
I found it really beautiful and it gave rise to so many thoughts. Wheelchair-user Emily Yates and her partner CJ decide whether they want to be parents and what it would mean for them. Practicality and perception.
I enjoyed it so much, it prompted me to write a few reflections:
What amazing parents these two would be – their strong relationship shines through. I love the humour, the depth of thought about the stuff that matters without overthinking the stuff that doesn’t; the sheer humanity
What a great way to explore a topic in depth, looking at it from different perspectives. Being real. What if Emily ended up as a single parent? What does it mean, as a disabled mother, to have a baby or for a child to be raised by a mum in a wheelchair?
Finding out how modern equipment can help. How brilliant that you can have a plastic baby delivered in a box and find out whether you can physically look after it – a bit like a Tamagotchi!
Societal attitudes. Stereotypes. The need to break stereotypes.
The Dad’s perspective. CJ is really keen to become a Dad, but will he ever be able to get out of the house again? But then don’t ALL would-be parents worry about how much their freedom will be curtailed.
Making clear that it is not all about worries that arise disability, but verbalising the worries all new parents have – how will I feel about the house being covered with poo and milk?
Availability of information. Why is there so little information to support disabled parents? What can we do about that? I’m sure some of our #MatExp community can make some good contributions here?
What an amazing series this BBC Sounds is – how lovely to dip into such a well-made piece of active research and get insight into other people’s lives.
Proud that our very own #FabObs Flo was the consultant obstetrician helping the couple on their way. So important to explore realistically what would be involved medically and find ways to support people to live their lives to the full and fulfil their dreams.
A really uplifting experience listening to this, and I wish Emily and CJ well with whatever life brings to them.
I don’t write blogs very often these days but sometimes, with just too many thoughts going round in my head, it is good to get it all down on paper. Or on a screen.
So please forgive/enjoy this stream of consciousness …
I have been an avid follower of Florence Wilcox’s fabulous podcast series, ‘The Obs Pod’. It is a year now since #FabObs Flo, my #MatExp partner in crime, first told me about the idea, having been inspired by meeting Natalie Silverman @fertilitypoddy at a conference, and I have been privileged to have pre-hears of the weekly editions.
Each one resonates with me in a different way. It might be my own birth experiences (yes, they stay with you for all those years) and now a proud Granny, or hearing Flo talk about her perspective on topics we have addressed through our #MatExp Whose Shoes work. The podcasts always give me deeper understanding of Flo’s thinking and what drives her in her mission to listen, learn and blend all the nuances of lived experience into her medical training and experiences as a doctor.
Anyway, the current episode ‘Ethics’ about the interface between medicine and what has traditionally been referred to as ‘fetal anomalies’ – a baby! – brought a flood of associations, memories and emotions. In particular, I thought of the wonderful network of people I have come to know and love over the last couple of decades. I felt proud that we have been able to contribute to a more human approach, with better information and choice for families from the point at which they are told that their baby has a higher chance of having Down syndrome; and then quality of life and acceptance and joy for growing families. This #TheObsPod episode brings together so many things for me.
Mel Smith and Grapevine are friends I have known for many years. Indeed, I attended their 25 year celebration (thankfully before the pandemic curtailed such activities).
Mel wrote ‘Imagine’, a fabulous poem about her relationship with her son Rishard as a very powerful contribution to our Whose Shoes event with the Coventry & Warwickshire maternity team in 2018. Hearing Mel read it here at the end of Flo’s podcast is just wonderful. I have followed Rishard’s progress and his dream to become an actor … including now starring in the BBC Doctors series!
I know/know of other young actors with Down syndrome. What progress they have all made over the last couple of years! Big shoutout to George Webster, starring in S.A.M and challenging societal stereotypes, including sexuality and learning disability.
I was invited to the Premiere in London of ‘The Peanut Butter Falcon’, for which Zack Gottsagen made Academy Awards history by becoming the first person with Down Syndrome to present the Best Live Action Short Film on The Oscars (2020). Such films really help people understand and embrace diversity, in all its many facets.
I was sad not to be able to go to the Premiere. And then in January 2020, I spotted the film in the film library on my way to New Zealand and it passed a very happy hour – a bit of a trip of a lifetime, just before the world went so pear-shaped. All these memories and associations come back by listening to a podcast on Ethics!
Enjoying Queenstown, New Zealand, before the world turned upside down in 2020!
Of the friends with Down Syndrome I have met through Grapevine, I must give a special shoutout to Heidi Crowter @HeidiCrowter95. Heidi is smashing stigma and stereotypes with her steely determination, resilience, courage, perseverance, joy, infectious giggle and firm belief that we can all achieve our dreams.
Heidi was a star of our #CovMindTheGap the movie’ film, which tells the story of our famous (infamous?) #CovMindTheGap workshop. So-called ‘hard-to-reach’ people queued at the door, took a full part in our Whose Shoes discussions before coming on our ‘Magic Mile’ walk. Complete with storytelling, dancing and singing in the streets of Coventry, this was one to remember.
Oh and by the way, Heidi got married last year – as people with Down syndrome do.
— Heidi Crowter-Living the dream (@HeidiCrowter95) January 6, 2021
Definitely @HeidiCrowter95 – young woman with Down syndrome, not only living the dream but advocating like a pro! Fighting for equality and squeezing in a wedding in between lockdowns! pic.twitter.com/3pFwfs1oYW
— Down Syndrome UK | Positive About Down Syndrome (@PositiveaboutDS) December 23, 2020
… Thinking of Coventry, my mind wanders back to ‘Our stories’ – my favourite-ever project in all my (#eek 30!) years working in social care in Coventry.
Authentic story telling – quite a story! I’ll keep it for my book …
My passion for personalisation was kindled by this project. We helped people with very complex needs to reclaim their lives through the choice and control afforded by personal budgets. We were successful in helping people to move back from extremely expensive (public services perspective) and miserable (citizen perspective – far from my family) ‘out of city’ placements. Unleashing this personal genie was a key trigger to me jumping ship from my day job to set up Whose Shoes.
I have a few spare copies of ‘Our Stories’ and have just sent a copy to Ghislaine Smith. Ghislaine is one of the current Darzi Fellows, doing a project in London to reduce the number of out of area placements for children and young people in care in the North West London. I met her at a #VirtualWhoseShoes session we ran in November 2020 with her #Darzi12 cohort. I find it fascinating how these different projects and connections wander into each other over so many years. I hope the booklet will be useful in some way, but learning from people’s stories never goes out of date.
… The local, regional, national and indeed international (especially now with such easy connectivity online) weaving effortlessly together …
Then there are all the friends I have met and experiences I have enjoyed through Nicola Enoch, Founder of Positive About Down Syndrome (PADS). I first met Nicola Enoch a few years ago when she attended our Whose Shoes workshop in Warwick. Well, what an amazing woman and story!
Nicola gave me a leaflet but I said it would have more impact if we took a photo and posted it on social media. I have since smiled seeing so many similar photos with movers and shakers in the maternity world: people Nicola has met through the #MatExp community. Nicola knows how to network and make things happen!
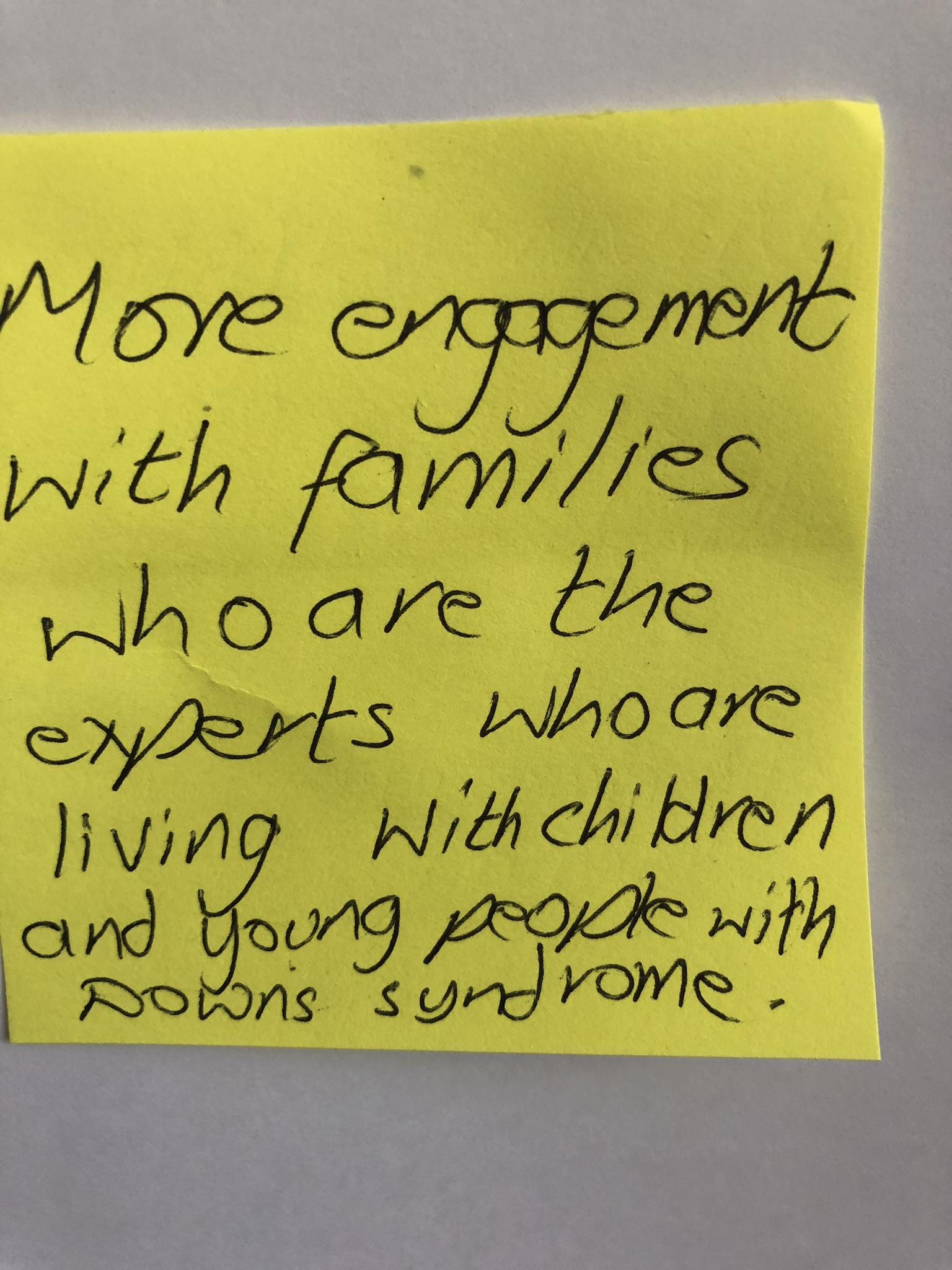
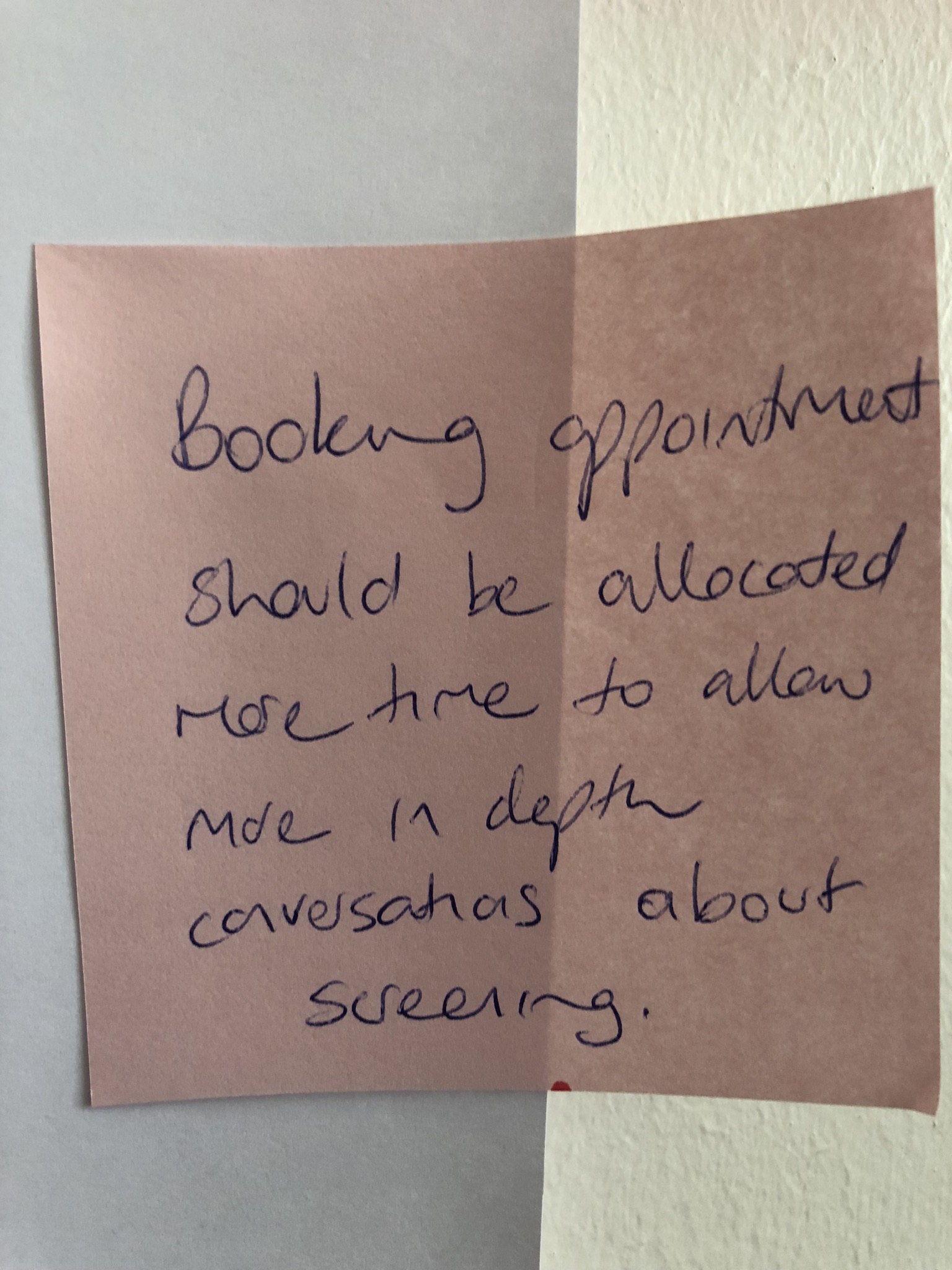
Nicola has helped me take forward work I started with Lewisham and Greenwich NHS Trust. Working with this innovative maternity team, led by Helen Knower, we had developed Whose Shoes scenarios exploring language used by healthcare professionals and experiences of parents and parents-to be around screening of Down Syndrome. Nicola became a huge champion of this work and attended a workshop with them.
Now Nicola and I plot and plan how we can best use our combined networks and resources to spread this thinking: Over 70 NHS trusts now have Whose Shoes #MatExp resources. Nicola has a vast network of parents across the country. We aim to get parents working with midwives, learning from lived experience, in more and more parts of the country.
We held a #DownSyndrome specific event with the maternity and neonatal teams at Coventry and Warwickshire NHS and have also been successful in inviting parents of children with Down Syndrome to join ALL our #MatExp #WhoseShoes workshops, meaning this important perspective is regularly heard.
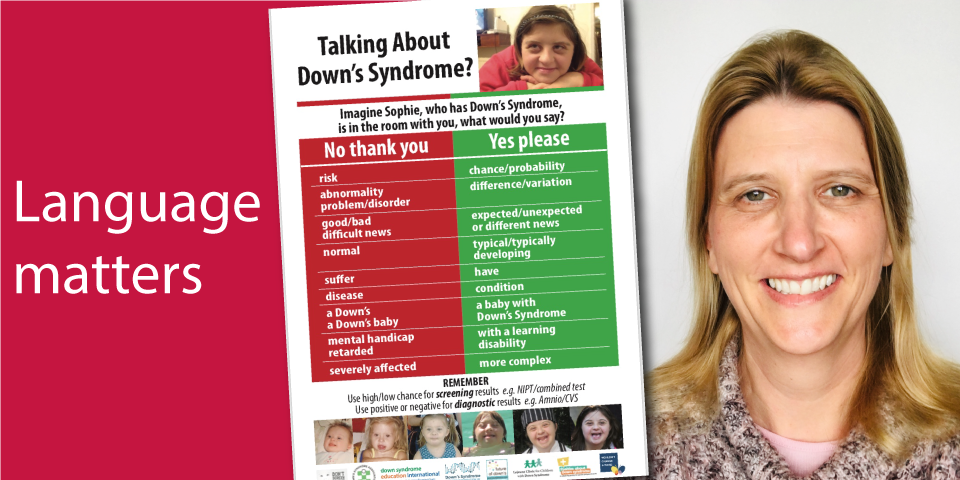
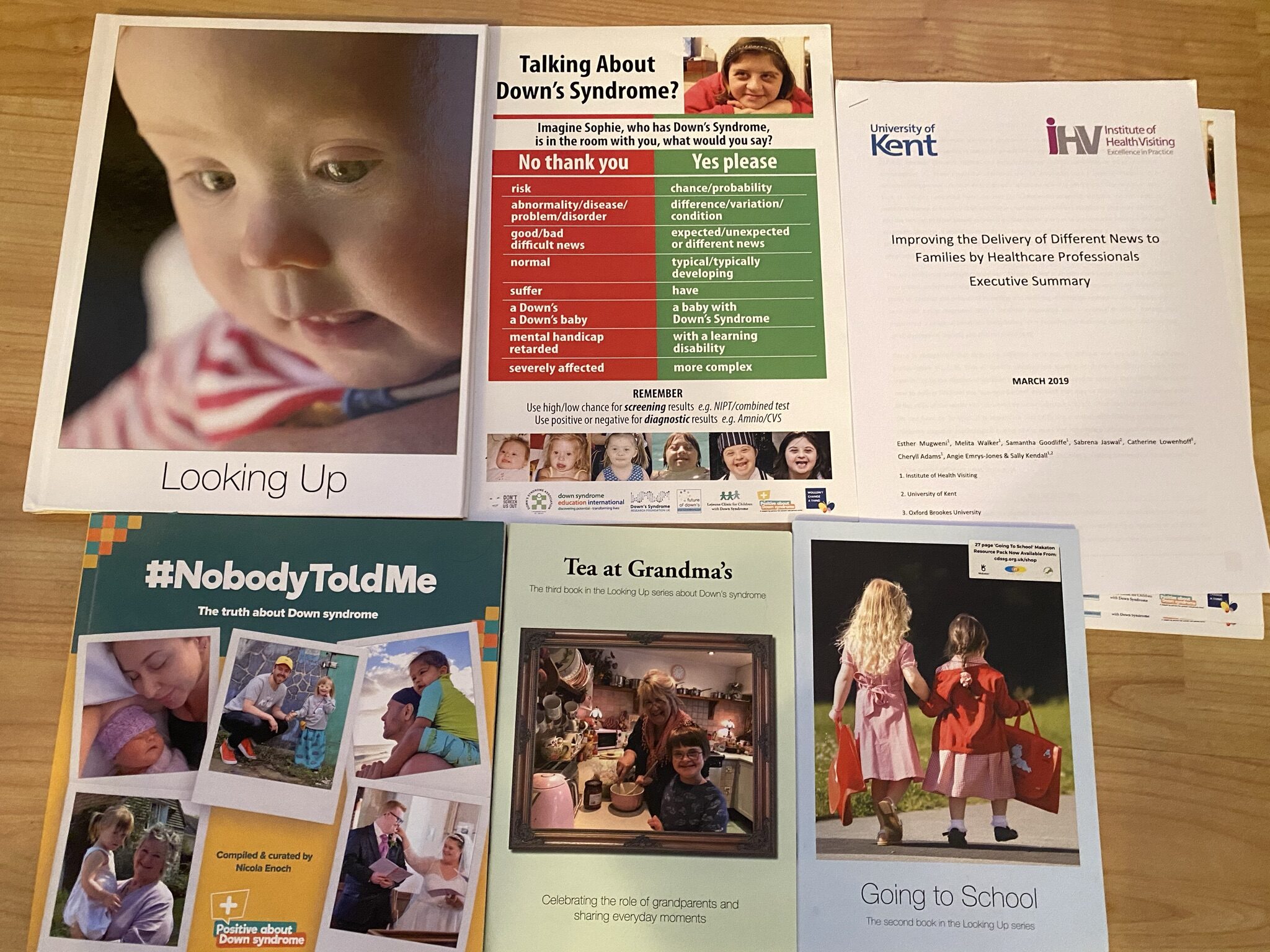
A highlight was when Colette Lloyd, an amazing Mum who spearheaded a campaign to re-think negative language around Down syndrome attended our Whose Shoes workshop with Barts Health NHS Trust. She caused so many ‘lemon lightbulb’ moments that she was invited to stay and run some training that afternoon.
Sarah-Jane Pedler
Teams like the maternity team in Cornwall, who really get Whose Shoes, have similarly done wonderful work in this area. I love following what they get up to in Cornwall. Sarah-Jane Pedler, a truly inspirational Professional Midwifery Ambassador and … well, everyone really (it is true coproduction) … hold an annual Whose Shoes workshop focusing on a different topic each time.
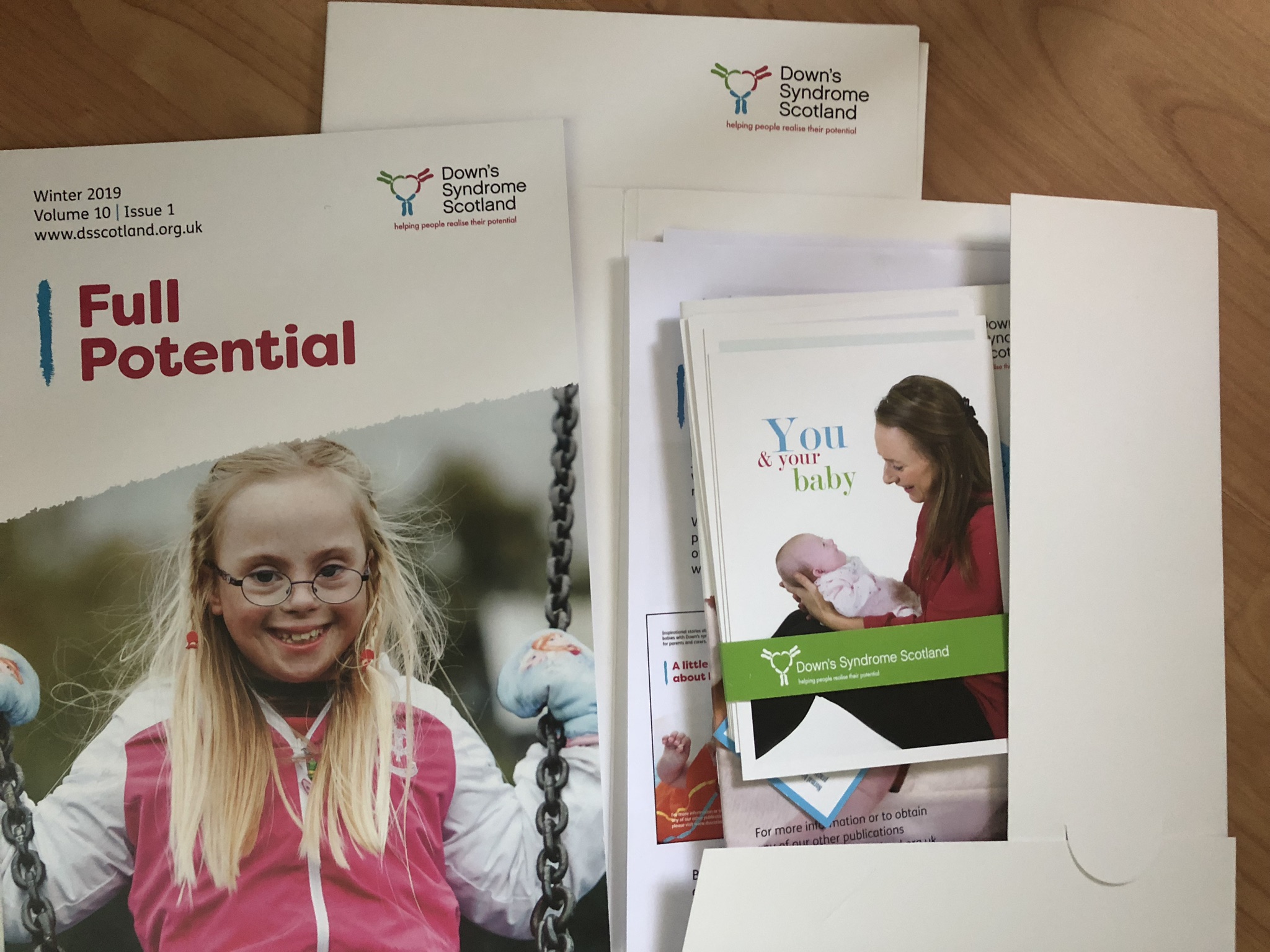
Angie Emrys-Jones @LookingUpBooks, who has a child with Down Syndrome, is Book Lead at Cornwall Down Syndrome Support Group. She has sent me some beautiful books. I’m sure they must massively help those they are designed for – reassuring images and stories about ‘Going to School’, and helping grandparents (‘Tea at Grandma’s’) and so much more.
It is lovely when people send me these fabulous packages. Another last year was from Nicola : the wonderful crowdsourced #NobodyToldMe book, full of positive images and stories of children with Down Syndrome. Flo refers to this in her podcast.
I knew Nicola‘s dream was to be able to influence the RCOG. How brilliant would it be to help shape doctors’ thinking right from the beginning of their obstetric journey!
Florence Wilcock introduces the Whose Shoes ‘Ethics’ session at the RCOG
Florence managed to get us a Whose Shoes training session with doctors at the RCOG. These people have huge influence in life and death decisions but may never have actually met a child or adult with Down Syndrome. Nicola embraced the opportunity to talk to them about the issues raised through the different Whose Shoes scenarios.
What a revelation to see issues through the eyes of a proud parent of a lively teenager, who happens tp have Down Syndrome!
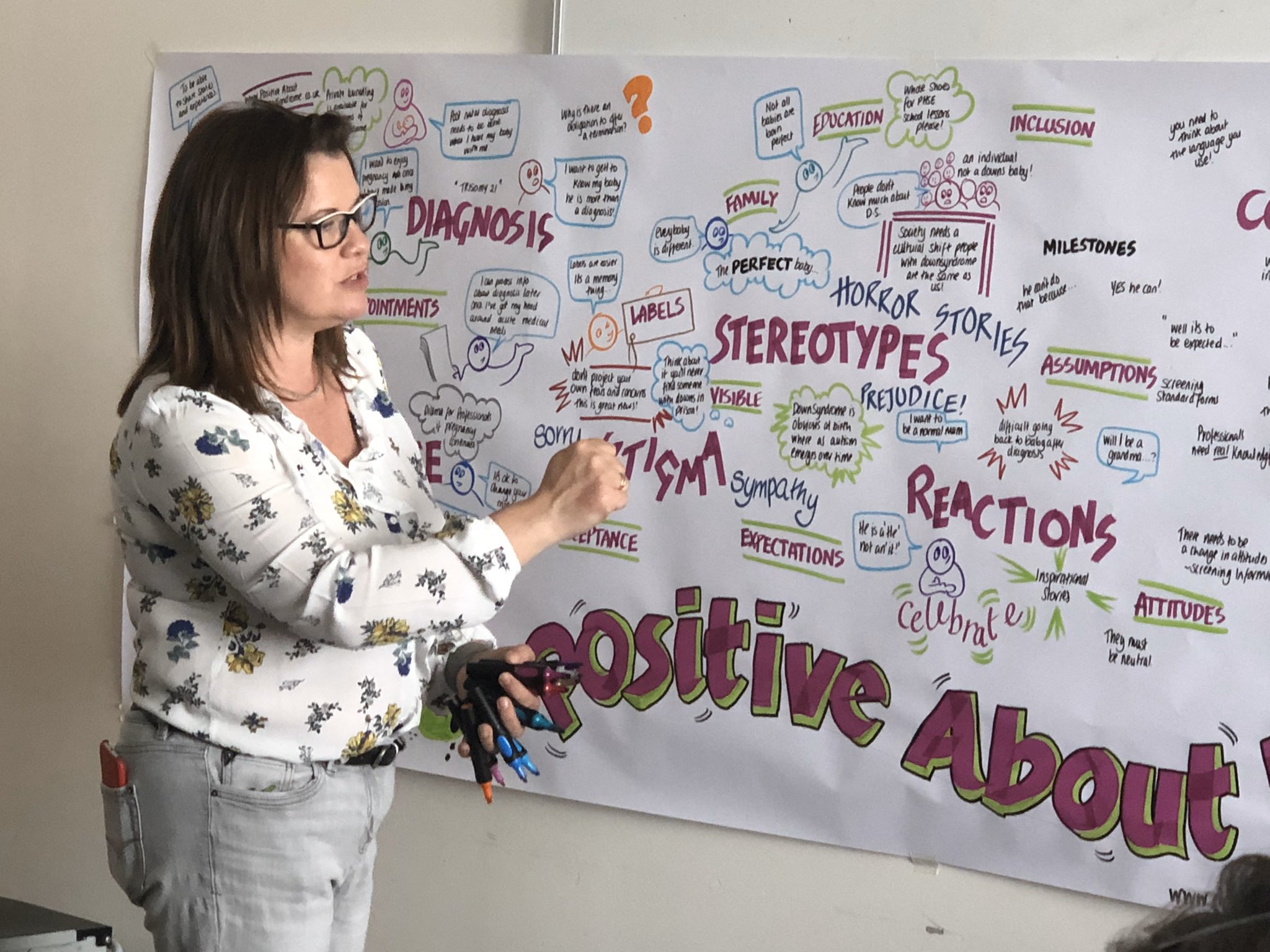
Nicola invited me to speak at her wonderful national conference for parents of children with Down Syndrome. Most of the speakers were parents; the agenda was packed. Every 15 minutes, a new (equally inspirational!) speaker! These people were wall-to-wall passion, leading initiatives and campaigns‘ (Don’t screen us out!’ and so many more). The energy of this #JFDI parents’ conference and the quality of the presenters will stay with me, which sadly is not the case for many far more expensive professional conferences I have attended … and indeed forgotten.
DS – Nicola’s conference 1
DS – Nicola’s conference 2
DS – Nicola’s conference 3 – Verity1
DS – Nicola’s conference 3 – Verity2
DS – Nicola’s conference 3 – Verity3
DS – Nicola’s conference 5
DS – Nicola’s conference 6 – Lynn Murray 1
DS – Nicola’s conference 7 – Lynn Murray 2
DS – Nicola’s conference 8 – Lynn Murray 3
DS – Nicola’s conference 9 – socks
DS – Nicola’s conference 9 Lucienne Cooper – socks
I have enjoyed networking with these parents. Meeting them in person around the country (and now joining our #VirtualWhoseShoes sessions). Lynn Murray @LynnAMurray joined the workshop up in Dundee. Colette Lloyd @ColetteLloyd joined our workshop in Barts in London, and immediately got invited to take part in some training that afternoon.
Wow, this is wonderful. One of the most #JFDI changes imaginable – a mum attending a #WhoseShoes session at Barts in the morning and delivering a session in a training course at Barts in the afternoon! Well done indeed Colette! #MatExp#impactpic.twitter.com/eQhni7Jntj
Sarah Sutton @peaponderer sang our #MatExp the Musical ‘Better births are here to stay’ song with us in Surrey using Makaton, while Caspar @N_Down_A_Caspar came along with his mum and stole the show.
And then the new passion emerging through all of this. Seeing student midwife, Verity Lancaster @LancasterVerity, student of the year 2019, giving up her Sunday to travel to the Midlands to speak at Nichola’s conference, talking about the work we first started at Lewisham and Greenwich and how it inspired her to lead in this area. Hearing her humility (‘just a student midwife’) but with more understanding and compassion than many far more experienced people; speaking from the heart.
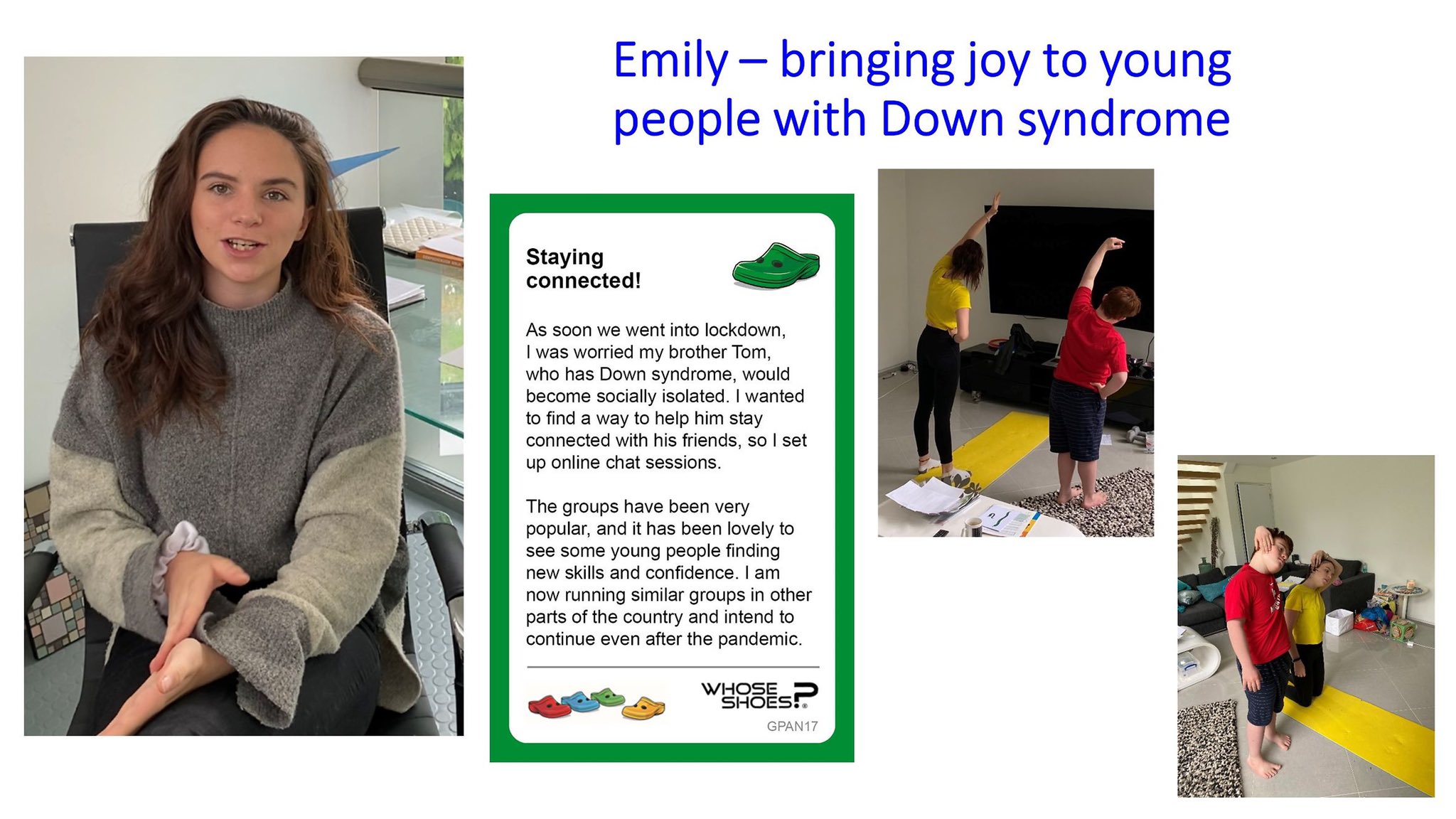
Being able to draw on this fantastic network of people and help showcase what they are doing is an ongoing journey. During the pandemic, Nicola‘s daughter Emily set up online sessions for her brother Tom and his friends, to reduce social isolation during the pandemic. These have now spread nationally.
We were delighted to help promote Emily’s sessions through the ‘Building the future’ #VirtualWhoseShoes work we did during the summer of 2020 and also in our recent Advent series.
I am now linking busy Nicola into discussions I am holding with ‘Wave for Change’, a wonderful organisation in London who are enabling people with and without learning disabilities to socialise together as equals. Which links back to my early connections with Grapevine Coventry, because it that is what they have always done.
And it was Claire Flower, a music therapist at Chelsea and Westminster hospital, who led the music extravaganza in #MatExp the Musical, on the main stage at NHS Expo, who introduced me to them.
Another inspirational mother is my friend Yvonne Newbold @YvonneNewbold – so much so, she was awarded an MBE in the New Years Honours list! Check out her webinars and her book, both of which help thousands of parents of children with special needs: The Special Parents Handbook.
And the networking continues … Dancing brings joy!
Indeed Gill! The @DanceSyndrome folks have been an inspiration throughout this pandemic. They played a huge part in @smallgoodstuff 's The Buzz too 😀👏👏👏👏🧡🧡🧡
Small people doing good stuff. I love the enabling work of @CommCats. They always help bring about amazing things in communities. The Buzz: a great collection of videos to help people stay active, engaged & inspired during #Covid19! pic.twitter.com/UaNHPGVCgt
In fact we all love Community Catalysts!! They make a lot of people very happy – like Grapevine and Wave for Change, helping people with and without learning disabilities to have fun together. True inclusion.
@CommCats Jen and I love you! Jen is so fulfilled just now – #downsyndrome – so what?! 💃is all that matters!
Celebrating #inclusion#diversity#dance and so much more besides. Would love to make these connections real. So great when every person feels welcomed and wanted.
It is great to see that Mel, Nicola and Yvonne have all endorsed Flo’s podcast episode on Ethics, saying that she has tackled a very sensitive topic in a compassionate, informative and non-judgemental way.
Ethics in maternity, including screening for Down's Syndrome, is always going to be a very difficult topic to discuss. Yet Flo handles it with grace, compassion, understanding & non-judgement. I wish every maternity practitioner & every parent-to-be could hear this. Thank you https://t.co/4mDp7jkDbL
Would urge all to listen & consider if their views/attitudes are influenced by last century or contemporary view of #Downsyndrome Thanks Flo 4 addressing this topic – attitudes & the law desperately need overhauling to ensure women can make truly informed choices knowing reality https://t.co/f3cJwHjVi7
— Down Syndrome UK | Positive About Down Syndrome (@PositiveaboutDS) January 9, 2021
Bridging the gap between services and people; shifting the power dynamics, promoting inclusion in the widest sense.
Yes, a lot of thoughts have been triggered by Episode 38.
Flo’s podcast has got off to a brilliant start in 2020, with thousands of downloads. I hope in 2021, it will become the go-to resource, with people not only subscribing to each week’s episode, but also dipping into all the richness that has already been created around a very human approach to obstetrics and maternity experience.
I am privileged to be part of this vibrant community focusing on what matters to people … which is really all that matters. Join us!
Ever since Flo first phoned me, back in 2014, asking ‘if Whose Shoes would work in maternity services’, I have been impressed by her person-centred approach, her ability to challenge the status quo and push boundaries and to work WITH women and families. She lives and breathes her powerful ‘Wrong is wrong …’ mantra.
‘The Obs Pod’ will appeal to everyone who has an interest in maternity services. Everyone will be able to take something away from each episode, due to Flo’s wide-ranging experience, gentle reflective style and ground-breaking practice.
Gill Phillips, Creator of Whose Shoes? and co-founder, with Flo, of the #MatExp social movement
As a young Mum who was totally blown away by the inspirational obstetricians who delivered my baby nearly two years ago, I am excited to start following ‘The Obs Pod’. The first episode was fantastic; so interesting and captivating. I am sure the podcast will be hugely popular with pregnant women and maternity staff alike, along with so many other people who will find it fascinating to gain an insight into the thoughts and experiences of someone who shares the beauty and intimacy of pregnancy and birth as part of their working life.
Jenny Thirlwall, young Mum and member of #MatExp community, West Midlands
One of the things I have enjoyed the most over the last five years of #MatExp is the opportunity to get creative. From being ‘just’ an obstetrician, I have branched out and added: writer, poet, facilitator, film maker, speaker, campaigner to name just a few new skills.
Gill encouraged me to write a blog. I promised my husband it would be just the one, resulting in a nickname now from Gill ‘One blog Flo’. as I have lost count now of how many I have actually written after dipping my toe in the water.
I’ve enjoyed making Steller stories after a quick demo on a train journey, particularly our #MatExpAdvent series and my Nobody’s Patient monthly project reports. I have made videos, my contribution to our series for #MindNBody launch being one of my favourites, reading my poem ‘Reassured’. All this is alongside my day job and I find these creative outlets re-energise me, develop me and feedback into my day to day working in maternity care.
In December, I was lucky enough to meet Natalie Silverman @FertilityPoddy at RCOG women’s network meeting in Manchester. https://www.thefertilitypodcast.com/ She talked enthusiastically about podcasting. She made it sound both interesting and achievable. Something that wasn’t too challenging but that might reach a different audience. She was inspiring and willing to offer advice. I went home enthused.
I spent the next couple of months thinking and exploring, I decided I have things I would like to share. Adam Kay’s book ‘This is going to hurt’ has been a runaway success, but I want to voice a different perspective of the maternity world. One that would be accessible to women and staff alike. One that might ignite change and action as well as entertain. So, I have rolled up my sleeves, listened to a podcast series on making a podcast, taught myself the lingo, attempted the editing and technical bits and loved every minute.
So here goes, I am launching my next adventure: The Obs Pod. I hope you enjoy listening as much as I am enjoying making it!
Flo
Here are the episodes so far and new ones will automatically be added here. If you wish to access the programme notes Florence refers to each week, find the episode you are interested in on The Obs Pod (buzzsprout.com):
On Monday, to begin #ExpOfCare week, we had an insightful blog from Dr Sarah Winfield reflecting on her experience of taking part in the ‘Lithotomy Challenge’. And today, to end #ExpOfCare week, another #FabObs, Dr Florence Wilcock – the originator of the #LithotomyChallenge and co-founder of #MatExp – tells us all about Caesarean sections and what really happens…
Dr Florence Wilcock
As we come to the end of #ExpOfCare week, I would like to share a blog about Caesarean sections, to demystify the birth that mothers and partners may unexpectedly experience. I originally wrote this blog at the request of Milli Hill & the positive birth movement in October 2016 , subsequently this has been included as a contribution to Milli’s book ‘The Positive Birth Book’ published 16th March 2016.
Why do we need to talk about Caesarean sections?
Unfortunately, sometimes people can be prone to making value judgements about different types of birth. One of the most common examples is vaginal birth = good and Caesarean section = bad. The truth is that in the UK current statistics show 25% of women will give birth by Caesarean section, 10% planned so called ‘elective’ and 15% unplanned ‘emergency’. We can argue these rates back and forth; we can aspire to improve care and change these facts, but for the moment given that 1in 4 women will meet their baby in the operating theatre it is vital that we talk openly about this experience and how it can be a positive, emotional & fulfilling birth for each new family.
Even in an unexpected ‘emergency’ there are still choices to be made. Nice guidance on Caesarean section CG132 section 1.4.3.4 recommends 4 categories of urgency; only category 1, the most urgent suggests delivery within 30mins. Far more common is the ‘emergency’ caesarean category 2, delivery within 75mins of decision making. This gives a woman time to express contingency birth preferences and ensure that even if she did not plan a caesarean birth it remains a calm and positive start for her and her baby. Skin to skin in theatre, optimal cord clamping, birth partner announcing the sex of the baby, choice of music are all possible. I would love to say these are all standard in every hospital but unfortunately that wouldn’t yet be true, however the more women know and ask, the more these will become universally accepted. As I often say ‘Wrong is wrong even if everybody is doing it and right is right even if nobody is doing it’. I wish you all an interesting and positive month discussing Caesarean birth and would like thank Milli for inviting me to contribute & become part of it. If you want to know more about how I am working to try and improve maternity services do check out matexp.org.uk
Caesarean Section a theatre experience & Who is who in the operating theatre?
The majority of caesarean sections in the UK will be done under a spinal anaesthetic, that is numb from the nipples downwards. It’s a peculiar feeling as one can feel touch but not pain. It means that women will be awake and aware of people milling around them which can be daunting but it also means they are awake and ready to meet their new baby. Lying on the operating table we tilt women slightly to their left to keep the bump of the baby off the major blood vessels, this prevents dizziness from low blood pressure. If you lie on the operating table in the maternity theatres at my Trust you will look up and find butterflies & cherry blossom on the ceiling, something nice to focus on while you wait for your baby to arrive. I know this is unusual & we are lucky but there is nothing to stop you tucking your favourite picture or photo in your birthing bag so that you have something familiar and relaxing to look at.
It might seem odd that at the start everyone in the theatre will introduce themselves to one another. It isn’t that we have never met but its start of the World Health Organisation (WHO) safety checklist. There is a special checklist just for maternity theatres and it is routine to start by checking simple information such as the woman’s name and date of birth and move onto clinical issues and equipment and it is all aimed at making the experience as safe as possible. So, who are all these people around you and what are their roles, why are there so many people there?
Anaesthetist: At least one sometime two; these are doctors who will administer the anaesthetic ad monitor you closely during the surgery. They will be standing just by your head and often chat to you and reassure you as the operation progresses.
Operating Department Practitioner (ODP): at least one; their role is to assist the anaesthetist, getting & checking the required drugs, drips or equipment, the anaesthetist cannot work without one being present.
Obstetricians: at least two; one will be performing the Caesarean section (the surgeon) the other will be assisting (the assistant) e.g. cutting stiches, holding instruments.
Midwife: At least one; to support the woman and help her with her newborn baby when it arrives
Scrub nurse or midwife: At least one; To check, count all needles, stiches and instruments and to hand them to the surgeon when needed.
Midwifery assistant or runner: This person double checks the swab and instrument count with the scrub midwife or nurse and ‘runs’ to get any additional equipment required as they are not ‘scrubbed up’ so can go in & out of theatre to fetch things.
Paediatrician: asked to attend any ‘emergency’ situation or if there are known concerns about the baby.
So, you see in theatre there is a minimum of seven people caring for any woman all with specific tasks to perform, any complication may result in us calling in extra members of the team.
So back to the woman, she will be on the operating table with her birth partner by her side and the anaesthetist and ODP close at hand. She can often choose the music she would like her baby to be born to. The anaesthetist needs to monitor her heart with sticky labels but these can be put on her back and her gown left loose leaving her chest free and ready for skin to skin with her baby. A sterile drape will be placed over her bump and this is usually used to make a ‘screen’ so that the woman doesn’t see and surgery she doesn’t wish to see however usually we drop this when the baby is ready to be born.
Many hospitals are starting to explore options of optimal cord clamping (waiting to clamp the cord) and passing the baby straight to the mother if the baby is in good condition. These can be done but need to be thought through so as not to contaminate the sterile surgical area, and the surgeon needs to be confident no harm such as excessive bleeding from the womb is happening whilst these things occur. Surgical lights need to be on so the surgeon can see clearly and operate safely but I know one anaesthetist who works in a hospital where the rest of the theatre lights can be dimmed. The mum and new baby can be enjoying skin to skin whilst the rest of the operation proceeds. Weighing and checking babies can be also done at this time but also can be done later on.
Traditionally if we operate with women under a general anaesthetic (asleep) her birth partner has not been in in theatre as their role is to support the woman. Recently on several occasions I have challenged this so that a baby is welcomed to the world with at least one of its family present and awake rather than by a group of strangers caring for the unconscious mother. There are safety considerations to be talked through for this to be successful but it is possible. However, kind and caring staff are, they are no replacement for a birth partner whom the mother has chosen to support her in the intimacy of birth.
I hope I have given you a brief glimpse in to life in a maternity theatre. As an obstetrician, I am privileged to help bring many women and babies together for those special first moments. The emotions are always different for me: sometimes it is a couple I know very well and have bonded with over months or years, sometimes a woman I have only just met who has had to put her absolute trust in me immediately. The theatre atmosphere can range from almost party like jollity to quiet intimacy. Every birth is different; each birth is extremely special just as much as the births that happen in a less clinical environment and each birth will stay with that woman forever.
It started with a thread about infant feeding that the lovely Lucy began on the #MatExp Facebook group. It was a fantastic discussion with a realistic and compassionate look at all kinds of barriers and problems, but one comment from student midwife Amy Prodgers stood out for me the most:
“Have found this discussion really fascinating as have been reflecting on similar issues after my first week on postnatal ward as a student midwife. I could go on about loads of things but a key point for me is the conflict between safe sleeping advice and facilitating breastfeeding. Women are exhausted from their birth experiences and their babies just want to feed but can’t sleep together. Women then end up feeling a failure for not being able to settle their babies in the cot, whilst also feeling guilty for wanting to sleep. This is when women start asking for formula and when midwives begin to doubt their intentions. Totally undermines confidence.”
I started a new thread with this comment at the top, and tagged in Gill Phillips as I felt it would make an excellent scenario for the WhoseShoes game that is used in #MatExp workshops around the country. We then had a discussion about bedsharing that raised some important points, and I felt it important to capture that discussion and share with you here.
An IBCLC on the group explained that “The old co-sleeper cots don’t fit the new beds (which were needed to reduce back strain on staff). However there are several new designs that fit the new bed, and research starting up too. Helen Ball’s research and videos of mothers clearly showed that the co sleeper cots made things *much* easier for mothers, much happier for babies, and didn’t add to staff’s workload.”
But would co-sleeper cots solve the problem? A paediatric consultant commented “I had co-sleeper cots after both my deliveries but actually my babies just wanted skin-to-skin for the whole first night. I think we really need better hospital beds in maternity and children’s wards to facilitate bedsharing.”
The important thing to bear in mind here is that these babies are displaying completely normal behaviours. It is our maternity wards that need to be “fixed”, not the babies. For a lot more discussion about expectations and reality when it comes to infant sleep, please see this blog by Alice Amber-Keegan of the Infant Sleep Information Source: https://growingfamilies.co.uk/2016/09/04/infant-sleep-expectations-and-reality/
Founder of the Positive Birth Movement, Milli Hill, agreed that “co-sleeper cots imply that at some point your baby will not mind being put down separately from you, and that you won’t mind putting them down separately either! Not always what mum or baby wants or needs.”
And of course, not having baby on the same surface as you can make life very difficult for post-birth mothers, as Polly Rogerson pointed out: “I was in hospital for a week after birth [due to post-partum haemorrhage], I was so weak that I couldn’t even lift my baby out of the cot – even with it right next to the bed. Yet somehow I was expected to do exactly that to try to feed him.”
Bedsharing when Baby is Unwell
The conversation then went in a couple of different directions – one discussion of bedsharing on children’s wards when a baby is ill, and one discussion of the guidelines that trust’s expect health visitors to follow when discussing bedsharing with the families they support.
Anyone who follows my hospital breastfeeding campaign will know how excited I was to have a paediatric consultant say that it would be good to have bedsharing facilitated on children’s wards! The consultant in question went on to say:
“Because in real life, I’d say close to 100% of families bedshare when children are ill. Banning it on hospital wards is just stupid. Having informed discussion about it is sensible.”
She clarified that her reservation for bedsharing with unwell children “is smoking parents and small babies and children with respiratory illness, as it is unrealistic to expect parents to stop smoking at such a stressful time, but the smoke clinging to clothes and hair definitely seems to exacerbate the children’s respiratory problems.” However this doctor confirmed:
“I spend a lot of time at work putting babies and children back into parents’ arms. That’s where they are usually happiest, but most importantly for me, most physiologically stable!”
This issue came up on my own private Facebook group today, as a member explained that her niece was hospitalised (and will likely be so for some time) and is refusing to sleep anywhere but on mum. As mum is unable to bedshare in hospital due to lack of facilities, mum is getting very little sleep.
A paediatric nurse on my group explained that from her professional perspective “we never advocate or advise co sleeping in our hospital as the babies are with us due to illness & therefore it can increase the chances of problems. However it is a parent’s choice and some still do, but we are bound by our duty of care to highlight the implications.”
She went on to say though:
“I’m a big believer in family centred care (which all children’s wards/nurses/professionals should be) so if a parent still wants to co sleep (and they would do so at home) I feel it’s my duty to help that parent as best I can so their wishes are upheld, but in a way that I feel most comfortable with in my work setting. As a children’s nurse you’re not only nursing the child but the whole family too, so to keep things as they would do at home or in regular life is important; the change of circumstance by being in hospital is bad enough for the child and family never mind then saying ‘well sorry you can’t keep your normal routine whilst here’. I think sometimes as a health professional we’re so focused on making that child better medically it can be forgotten how big a change being in hospital can be on them emotionally; even though they may not outwardly show signs of distress it is definitely affecting them psychologically, and therefore keeping things as much to their norm as possible is very important.”
Bedsharing when Baby is at Home
Image courtsey of Beverley Latter and the Infant Sleep Information Source
The discussion about what health visitors can and can’t say to new parents was prompted by one mother explaining “my health visitor at 6 weeks (1st baby) gave me info about safe co-sleeping and it was the reason I continued to breastfeed.”
I then shared the discussions that mothers from my group have had with health visitors online, including a discussion specifically about bedsharing: HVe-COP newsletter The two quotes from that discussion that summarise the issues for me are:
“We are very constrained sometimes. We have to follow Trust policy…..even if we believe that bed sharing can be very beneficial and are up to date (with evidence)” (health visitor participator)
“Just to put this out there…….we have a responsibility to our NMC Code of Practice and the clients…after that Trust policy is important. The day health visitors do not provide evidence based information to their clients because of Trust policy is a grave one indeed” (health visitor participator)
On this thread in the #MatExp group, one health visitor explained: “Trust guidance is the Lullaby Trust safe sleep recommendations, and signposting to NICE for bed sharing…..personally I don’t advocate it but I talk about if [you are] bedsharing [how to] minimise risks.”
This conversation took place before the launch of the new Baby Friendly “Co-sleeping and SIDS” guidance for healthcare professionals, which has been developed in conjunction with the Infant Sleep Information Source and the Lullaby Trust. This guidance focuses on helping healthcare professionals “to take a sensible, proportionate parent-centred approach in order to find practical solutions to this complex issue”.
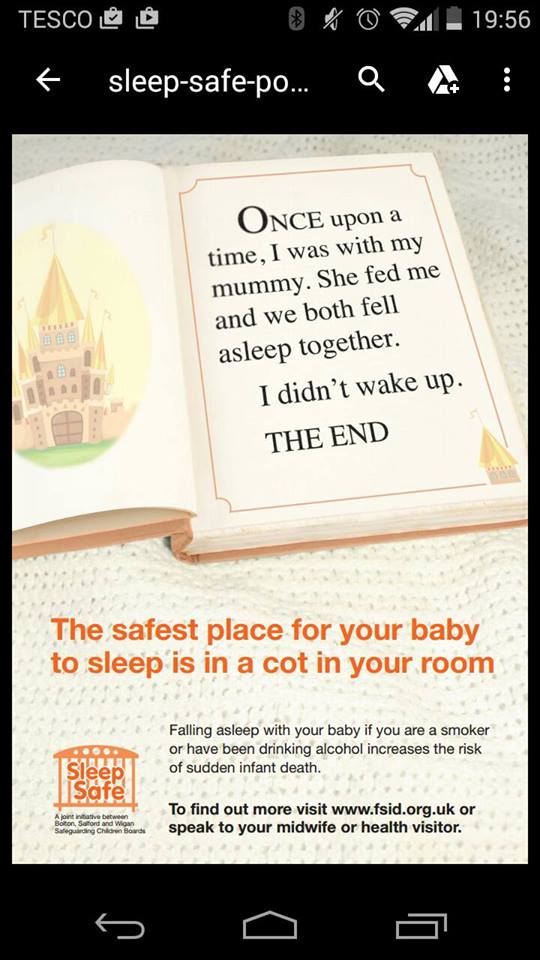
We can hope that this guidance and the continued expansion of Baby Friendly training for UK health visitors will put an end to less nuanced campaigns such as this one from Bolton, Wigan and Salford that Amy Prodgers highlighted:
As you can imagine, this heavy handed campaign elicited a strong response from those on the thread! Amy herself commented that “reducing SIDS by telling people not to bed share is a bit like reducing road traffic accidents by telling people not to use cars! And of course we’ll also avoid the issue of how much more dangerous it is to fall asleep on the sofa (whilst presumably trying your best to follow this advice and stay awake).”
One mother’s experience explains the reality of what happens when health visitors advise against bedsharing: “When I told my HV I was co-sleeping, on purpose and in accordance with safety instructions, she gave me leaflets on ‘cot death’ and strongly discouraged me from doing it. She then arranged another visit for a few weeks later, after advising me to ‘keep trying with the moses basket’. When she returned I just lied and said that my baby was now sleeping in the basket as I couldn’t be arsed with having to defend my conscientious parenting decisions.”
Midwife Sally Goodwin said at the end of the thread that she was “grateful to all for highlighting this issue. I think this subject comes up erm…… every day for me as a midwife.”
Certainly a topic we need to continue to discuss then.
I was asked to do a talk to student midwives at Salford University in January on the topic of “Women’s Voices” in maternity care. As part of my presentation I included the voices of the midwives who work in maternity care, and a reminder that there are many other women for whom maternity care is their professional, as well as perhaps their personal, experience. “Women’s Voices” in maternity care should cover the midwives, obstetricians, health visitors, doulas who care for us, as well as the women giving birth.
So I decided to start a series of blog posts on “Women’s Voices in #MatExp” from the point of view of those working in maternity, and this is the seventh of those. This is Fleur Parker’s experience as an antenatal teacher – thank you so much to Fleur for agreeing to write for us. You can read the other blogs in the series here:
And yes, I will be doing a “Men’s Voices in #MatExp” series too. Because this campaign is about all voices.
Helen.x
*********************
I am putting my head above the parapet to say I am an Antenatal Teacher.
I’m not sure why, but recently we have been getting a lot of flak. Sometimes it feels as if everything that is wrong with birth is the fault of the antenatal teachers. On Twitter famous names berate us and newspaper columnists lampoon us
So writing this piece is taking quite a lot of courage and I hope I can do us proud.
There are many, many antenatal teachers – those of us who work with expectant parents during pregnancy to help them prepare for labour, birth, the fourth trimester and the early days as a parent. We come in different sizes, shapes, colours, languages and approaches. There is not a one size fits all approach.
There are three ways to prepare for labour and birth – intellectually, physically and emotionally/mentally. In my experience it is those who prepare a little every day in each of these ways that feel most able to cope with their labour and birth experience. There are a lot of options for antenatal preparation – yoga, pilates, aqua natal, hypnobirthing, NCT classes etc.
I have absolutely no idea why I am an antenatal teacher. I didn’t go to antenatal classes myself. My son is now 20 and I think I’ve finally come to terms with the fact I am a Mother – I will not be the first in the queue to cuddle your newborn. I will however, have freshly baked cake and a lovely cup of tea and all the time you need to talk, explore and work out what the £$%^@* just happened.
I support men and women, over 1,300 have attended antenatal classes I have facilitated. First time mums, fourth time dads, same sex couples, single mums, surrogate mum and dads, young mums, old mums, surprised mums and reluctant dads. We’ve all sat together, in a circle not knowing quite what to expect.
I have taught classes on my birthday, my husband’s birthday and my son’s birthday. I’ve taught when I’ve been happy, sad, ill and well. I’ve sat before a group after finding out my mother-in-law had died, unexpectedly on the operating table, on Christmas Eve and there was still four hours of a six-hour class left – and not told them because it isn’t about me.
It isn’t about my birth experience (caesarean in case you’re wondering) and there isn’t an NCT way to have a baby (whoops I’ve let the cat out of the bag I am an NCT antenatal teacher). The way to have a baby is the way that’s right for you, in the moment.
If I have an overarching aim as an antenatal teacher it is to disrupt the story of birth. To take the perceptions of expectant parents and give them the tools and skills to reimagine, to question and to put a story together that belongs to them – nobody else. By the time people are having babies they have heard at least a couple of decades of birth stories – perhaps it’s Daphne on Neighbours whose water’s broke, contractions started and she gave birth ten minutes later still wearing her tights and with Bouncer the dog sniffing around. Perhaps it’s a documentary, a soap or in films – there is a whole generation who have grown up with the story of pregnancy and birth from Twilight!
I hear hundreds of birth stories and often as I listen I’ll be thinking ‘okay, yes I could do that, it sounds hard work but okay. I understand that and it was straightforward enough.’ But the new parent telling their story is in tears, sometimes shaking and upset. Another time the story I’m hearing is one that shocks me, where I am, quite frankly, horrified. In this case the mum or dad is happy ‘oh it was great, we had a chat with the Dr and decided to do this and that and when that didn’t work we went for the other – oh and the blood!’ It’s not hysteria or false memory it’s just that they were okay with their experience, it was, in the moment, entirely appropriate.
The research shows us that that is what matters to new parents. It is less about the actual birth or in many ways the outcome but their satisfaction of their experience and perception of outcome that is most important.
There are also parents who because of the actions of others are traumatised and angry with the care they received – feeling abused and violated. I’m not sure any of us can prepare for those eventualities. Those are the parents I spend most time with, talking, understanding, signposting …… simply listening.
During classes we share stories, knowledge and experience. We look at straightforward physiological birth and we look at birth that is anything but. We think about becoming parents, relationships, cognitive, physical and emotional development of babies. We play nappy roulette (sometimes I like to fulfil the NCT stereotype) and speed parenting. We laugh and we cry and we eat cake.
I love my job – it is my passion and my purpose and I bring to it my head, heart and soul. I make lasting connections with people who are entering a whole new phase of life and I walk alongside them.
I don’t have the answers and I don’t always get it right. But I have a lot of knowledge, rigorous CPD and I am an experienced and skilled adult educator and group facilitator. But I am not the answer and I am not the problem.
I was asked to do a talk to student midwives at Salford University last month on the topic of “Women’s Voices” in maternity care. As part of my presentation I included the voices of the midwives who work in maternity care, and a reminder that there are many other women for whom maternity care is their professional, as well as perhaps their personal, experience. “Women’s Voices” in maternity care should cover the midwives, obstetricians, health visitors, doulas who care for us, as well as the women giving birth.
So I decided to start a series of blog posts on “Women’s Voices in #MatExp” from the point of view of those working in maternity, and this is the third of those. This is El Molloy’s experience of supporting breastfeeding. Thank you so much to El for agreeing to write for us.
You can read the first two blogs in the series here and here. And yes, I will be doing a “Men’s Voices in #MatExp” series too. Because this campaign is about all voices.
Helen.x
*********************
I am an NCT Breastfeeding Counsellor in Coventry, and a Peer Supporter on the Infant Feeding Team (run by Coventry City Council). I sit on our local MSLC (Coventry and Rugby CCG) and was a member of the Coventry Breastfeeding Strategy Group. I am also a Babywearing Peer Supporter for Coventry Slings, and am about to do my Consultancy through Slingababy at some point this year. Probably after I finish the dissertation for my MSc in Child Health (through University of Warwick). I also help to facilitate the Coventry NCT Birth Choices (after caesarean or traumatic birth) Group after it was set up and run successfully by one of our amazing local Antenatal Teachers.
This is supposed to be a blog about Breastfeeding Support. Which means it also has to be about being a Peer Supporter – and being a Breastfeeding Counsellor. And now I don’t know who knows what those roles entail, or what we do in either of them. Is there a difference? Can parents tell the difference? Do they care? To be a Peer Supporter, or a Breastfeeding Counsellor – that is the question…I think?
I make a damned good cup of tea (and coffee – because I drink a *lot* of coffee). And at a push I can do cake, but usually I have biscuits. However this is all the icing on the cake or at least bribery, to encourage new mums to come to our groups, have a drink, have a biscuit, and stay a while. Let us listen to your story. And I carry tissues in my bag – always.
As a peer supporter I have had UNICEF training in breastfeeding support (for most projects this is between 6 and 10, 2-hour sessions, delivered by someone who may be the local Infant Feeding Lead Health Visitor or Midwife/IBCLC/NCT Peer Support Trainer). I am a mother who has breastfed her own children. If you want to get technical I *am* a peer supporter – I am still breastfeeding my youngest. I can walk alongside you in your journey, I can tell you that things were and are occasionally tough for me – that despite the official badge and t-shirt (purple this time round, blue before – I declined the hot pink – it clashes with my hair!) I am not an “expert”. I don’t know all the answers – and I’ve yet to meet anyone who does. But as a peer supporter I can tell you what ‘normal’ breastfeeding should look like. I can tell you that there are no rights or wrongs, except what works for you and your baby. With the caveat that baby is happy and you are not in pain. And I can offer you information about what you need to look for in your babies feeding patterns so you can feel confident things are going well.
Does Peer Support make a difference? I’d like to think so – and I can see locally that overwhelmingly most families find us useful. There are always the other stories, the one about the PS who said to use baby rice at 4 months, but that’s no different to the story about the Midwife who said baby should sleep for 4 hours between feeds, or the Health Visitor who suggested controlled crying… One poor piece of information shouldn’t tarnish a whole section of support. This is something we are seeing every day on #MatExp. There is a world of difference between midwives and *this* midwife; between Peer Supporters and *this* Peer Supporter. And the supporters are only ever as good as their training and ongoing Continuing Professional Development (CPD) and supervision.
And this Peer Supporter is also a Breastfeeding Counsellor. Specifically, I am an NCT breastfeeding counsellor. This means, for the uninitiated, that I am trained in person-centred counselling skills, that I am a sign-poster to other information, other options, other Health Care Professionals. But that always the mother is front and centre. This too means that I have breastfed my own children (for a minimum of 6 months – though extenuating circumstances may apply for others). It means that rather than the UNICEF training, I have spent 3 years distance learning through a University accredited course, writing essays, going on weekend workshops. Debriefing my feeding experiences; embedding my counselling skills in practice as well as theory, understanding and training in group facilitation (for both antenatal sessions on courses, and in running breastfeeding groups). Parents aren’t interested in the Diploma that I have, or the ongoing CPD that I have to fulfil, including regular supervision, or the fact that my CPD is specific to each of my roles within NCT. Parents just want to know what I can advise – what I can do to ‘help’. The honest answer is “nothing”. Because in either of my roles, that is not part of my job description. Advising would indicate that, again, I know best – and I do for me, but not for you. I have being trained as a reflective practitioner, and I have recently realised that I have moments of conscious and unconscious competence – I am, as we all are, a work in progress.
If I am visiting you, or welcoming you at our group, I will sit and listen to you talk about your options, and maybe offer suggestions. We might talk about how you feel about what you’re being asked to do, until you come up with a plan that is going to work. Reading the previous blog by Maddie, some of her descriptions about working with parents in labour – asking – what do they want to do, how do they feel… This too is how we work. And the general mistrust by other HCPs feels all too real.
As a peer supporter. I might come to your house on day 1, or day 2 after your discharge. Maybe you called, maybe your midwife referred you because she thinks you need a bit more time, someone to sit while you feed, time that she just hasn’t got because her caseload is so much higher. I fill in forms, I offer to register your child with your local Children’s Centre. I will ask you how your birth was (because this might affect feeding). Maybe your Health Visitor has referred you because you are 12 days in and feeding still isn’t ‘right’ for you. Perhaps your baby still isn’t back to birth weight. We have time. I have time to stay to the end of the feed and see how your baby slips down because the cushion could be in a better place…
As a Breastfeeding Counsellor I also have time to sit and listen to your worries about how feeding didn’t work well with your older child. You might have called me because I facilitated your antenatal session; or maybe you’ve been searching on the internet. You might have called the national line, and they have given you my details. Maybe you have come to the Drop In that I run with another colleague. I might visit you at home, where you apologise for going round in circles about whatever is worrying you – but I sit and listen, and reflect your words to you, or maybe ask the one question, or make the observation, that triggers the understanding in you that your worries are not all feeding related, that you’re concerned about your relationship with your partner.
I too go home and worry; did I say enough, not enough. Did I miss a subtext. I am all too aware of the responsibilities that the midwives and health visitors have. The understaffing, overstretching. We will refer in parents who are struggling. “If you are still concerned talk to your midwife, is this something you feel you can ask your Health Visitor about…”. We will make the phone calls where we are concerned about parents mental health, those feelings where things just feel slightly ‘off’. We trust that you will support families, and we ask that you trust us to do the same. Trust that we have the experience with breastfeeding, that we can and do support mothers long after they stop attending baby weighing clinics, long after their regular assessments – all still breastfeeding. We support them to continue, and to stop when that’s right for them. At 2 months, or 2 years, or even longer.
I want (I want?) I can say it in this context… I want all women to have confidence in their decisions, and to have the right information for them to make the decisions that work for their family. Whether that is because they understand that breastfeeding past 9 months isn’t tantamount to child abuse (yep, that old chestnut); or whether it’s because I signposted her to the information they needed about their anti-depressants which meant they had confidence in continuing to feed even when she felt her world was falling apart. Whether that’s because we worked on positioning until she finally hit that sweet spot and it finally clicked that no, breastfeeding does *not* have to be painful; or whether after seeing 6 other HCPs and being told that she had ‘forgotten’ how painful feeding was, I mentioned tongue tie as another possibility, and lo and behold division did result in huge improvements. We have time, I tell the women I see, don’t worry (often as I’m glancing at the clock, thinking, I’m going to be late to my last visit, and I know that’s 20 minutes away, and it’s already 4.45pm on Friday, and I finish in 30 minutes). When baby won’t latch, or has just fed before I arrived and won’t be woken. “How have things been?” “What have you tried?” “Some parents find…” I joke that all babies sleep for me, except my own. We talk about previous miscarriages, we talk about the joy in feeding her firstborn, and the fear that it won’t work this time. That she’s been told it’s just a “small” tongue tie, but she’s worried about him swallowing blood; we talk about how to deal with engorgement, and how can she ease the cramps that accompany her let down. How can her partner bond with baby, so when can she start expressing; we talk about shared bath times, and babywearing. And how will she cope when he goes back to work. We have such a fluid society that we don’t often live close to our mothers, and can’t learn from them the way we used to. My visits span the world, from South Africa to Vietnam, to Latvia, Canada or Scotland. The accents change but the worries and fears are all the same.
It gets easier, you can do this. And particularly in the light of the media frenzy unleashed by the Breastfeeding Series published by the Lancet. We can do this. Together we can change the world.
This post is from Michelle Quashie, and originally appeared on her blog site Strong Since Birth. Our thanks to Michelle for agreeing for it to be reposted here.
The day had finally arrived! After contributing to #MatExp and interacting with many conversations surrounding ‘WhoseShoes’ throughout the year, I was finally going to experience the magic in real life.
Laura, the chair of our MSLC has written a fantastic post that captures the excitement of the day perfectly, you can read it here: When WhoseShoes Came To The PRUH
I was not disappointed, the day was everything I had dreamed of, but for me it was so much more.
I was asked to open the event by sharing my Maternity Experience. I have spoke at several maternity training events in the past but my audience has always been Midwives. I was aware that this was a multi discipline training event and it was to be the first time I would share my story in such detail with Obstetricians and everyone else involved in Maternity. The thought made me feel anxious but I knew how important this opportunity was.
I had planned to stay in control and not let the emotions attached to my experience be displayed in the form of tears. It was so important to me to remain composed and in control.
My heart pounded through the showing of the MatExp film, this film moves me every time. It is so powerful and very thought provoking. Sadly I can resonate with many of the situations displayed in the film. I knew I was about to be discussing some of those memories any minute with all those surrounding me.
My name was called and I made my way to the front with my heart pounding. I decided to be honest and share how I was feeling with the room.
‘Please bare with me, I am feeling very nervous. I’m sure once I start talking I will warm up and I will be fine!’
Automatically I felt more relaxed and felt more able to share my story without the anxiety overruling my thoughts.
It’s amazing how every time I share my experience it comes out slightly different, or I find myself saying things that I hadn’t thought of before? I had missed a couple of important bits out but neither the less I was very happy with the way I had presented and gauging by the feeling of emotion in the room I had touched the hearts of nearly everyone around me. For the first time I was able to keep my tears to myself even though I had noted that tears were shed by many in response. The room fell silent but the atmosphere spoke volumes.
I wasn’t aware of the tweets that were being circulated on social media but looking at them them later along with the emails I had received It confirmed that my talk was a positive part of the day.
“Also a massive well done to Michelle for her heartfelt and emotional story, I could see it touched many people as there were certainly a few tears in the room. That took huge courage to stand there in front of so many people and share such a personal experience and to tell it so well. Huge WELL DONE Michelle.”
We began to play the the game and interesting discussions were had in response to the thought provoking questions that are key to the WhoseShoes success.
Some of the discussions that stick in my mind were:
A woman wanted a home birth but her husband wasn’t convinced. We had discussed that there wasn’t enough support or information given during antenatal care to ensure that the couple felt safe,supported and empowered to fulfil the woman’s birth choice.
Consultant Obstetricians are normally addressed by other members of their team using their title i.e., Sir, Mr, Mrs or Miss as a mark of respect. I may be wrong but it feels hierarchical, unlike the power slogan and barrier breaker behind WhoseShoes and #MatExp ‘No Hierarchy, just ordinary people’.
It was also discussed that consultants were on site until 9 pm, after that they are on call for emergency situations only. Now I understand why during my appointment to discuss my VBAC, the registrar said ‘ I mean, we don’t know when you will go into labour or who will be on duty should you rupture’. I now understand that my birth choices were influenced by staffing levels at the hospital.
Other key themes were Empathy, Language, supporting and facilitating informed decision making and just how important it was for everyone to be cared for individually based on their individual situation and needs.
Midwives are able to have time to build a relationship with women whereas doctors are often called for the emergency situation and do their best to resolve the medical issue as it arises. This can sometimes make it hard for them to be able to connect with the woman that they are caring for and are not always able to fully appreciate the long lasting effects the experience can have on a woman.
The day was coming to an end and Anna gave us fabulous evaluation of our morning using the comments that came from the discussion at each table. It was fabulous to visualise the discussion using the graphic that Anna had been working on through out the morning.
We each made an individual pledges. Here is my pledge:
“To provide a platform for women to share their Maternity experience. I would like to ensure that women’s voices are heard as part of training and development.”
I am currently planning a conference called ‘Women’s Voices’. More details will be available soon.
As the morning came to an end and people were leaving someone tapped me on my shoulder. I turned round and my tummy flipped. The face before me took me straight to a place of feeling vulnerable, feeling panicky.
‘Michelle it was me wasn’t it?’
Stood before me was the registrar that I had my consultation for my vba2c with. Unbeknown to my self and the organisers we had shared the morning. I had shared an experience that changed my life but had also been a time that left me feeling scared, vulnerable, isolated and questioning my mental health. The person that was responsible for those feelings was standing here in front of me, for a moment the feelings came flooding back, I battled to keep them contained.
She apologised for the way she had cared for me. She admitted that she had been wrong and has since ensured that she was fully aware of her professional guidance. She was now fully supportive of women’s choice regarding their birth and ensured me that since having to write a statement in response to my complaint, she is fully aware of the impact of the care she provides a woman.
She actually thanked me for highlighting the error of her ways promising me it had changed her attitudes. I could see that she was overwhelmed with emotion and had spoke to me honestly. She asked if she could hug me and we both held each other for comfort.
I told her that I admired her for taking the time to come a talk to me and for apologising. I also explained that I was aware that she was not entirely to blame for the care I had received and I now understood that her response to me wanting a vaginal birth after two caesareans was due to the cultural belief of the trust she worked in.
It was clear that my birth wishes would not be supported and neither would anyone wanting to support me at that time. I know this because many attempts were made to provide me with the support I needed and no one stepped out of their comfort zone to provide me with the support I needed with regards me birth choices. As a result I had no choice but to transfer my care.
She empathised and promised me that as a result of my experience things were changing.
We said our goodbyes and I was trying very hard to contain my emotion that the meeting had evoked.
A consultant midwife that has walked by my side through this maternity experience and others and who has been a pillar of support to me came to see me. ‘Are you OK Michelle?’
The flood gates open and I broke down. I couldn’t talk at that moment. I was just overwhelmed with emotion. I couldn’t make sense of it at the time but now I think I can.
That meeting with the registrar brought some closure. I admire her ability to acknowledge the error of her ways.
The meeting took me back and reminded me of the scared women I once was sitting in her office, trying to persuade her that I could give birth, pleading with them to allow me. Feeling so horrible when it was highlighted that I had never given birth and they wasn’t sure if I could. I was subjected to a number of negative comments that effected my mental well being and left me questioning my sanity. Comments that left my family feeling unable to support my decisions in fear of my safety. it was a meeting that left me feeling isolated.
Here I sat after coming full circle with the same women but this time I was a different woman. I am a now a woman who has had the most amazing journey and have achieved some incredible things;
I gave birth, not only did I give birth but I bloody rocked that labour ward!
I came back and I told the story, I sang it from the rooftops!
I learnt to believe in me and my abilities.
I joined their MSLC and contributed to so many fantastic improvements within the Maternity service.
I have spoke at training events within maternity with an aim to improve maternity care for women.
I have written and had my views published here and in The Practising Midwife .
I have contributed to #MatExp campaign and connected with some fantastic people as a result.
I have met, received support and been inspired by many fantastic people. too many to mention.
The realisation that my shoes have climbed a mountain has happened!
I received the following email from a Consultant Obstetrician following the Whose Shoes event. It confirmed that this journey has been worth every little step:
“Dear Michelle,
I just wanted to reiterate how touched I was by your story and how impressed I was by the way you delivered it. You will be responsible for improving the practise of every obstetrician in that room today which in the end will improve the care of tens of thousands of women.
I have great pleasure in introducing a guest blog from Kirsty Sharrock, a.k.a. SouthwarkBelle. Kirsty is mum to two girls and lives in London. Her other day job involves biological samples, powerful lasers and badly fitting lab coats. When her first child was born in 2009 she became fascinated, and often infuriated, by the amount of misleading information aimed at new parents. Her response was the SouthwarkBelle blog where she tries to make sense of some of the dubious science or at least have a good rant about it.
Thank you so much to Kirsty for writing for us on the topic of Induction of Labour.
Kirsty Sharrock – SouthwarkBelle
It’s a well known fact of modern childbirth: Inducing labour sets off a chain of other interventions which often result in an emergency caesarean.
But is this actually true?
Would you be surprised if I said it’s not? I certainly was. The idea goes against so much that I had heard from other women and from midwives, my antenatal teacher and of course the internet.
When I went overdue with my first baby I dreaded being induced. I’d heard nothing but horror stories saying it was entirely awful and unnecessary, it would almost certainly make the birth more painful and complicated and would probably set off a “cascade of interventions” leading, with grim inevitability, to the one thing I was most afraid off – an emergency Caesarean. It would also completely scupper my plans for a natural birth in a midwife led unit. But at the same time I was MASSIVE, it was August, and hot, I was desperate to meet my baby and had had quite enough of being pregnant. So I agreed to book an induction, then did everything I could think of to make that booking unnecessary. In the event I got my wish, sort of.
41 weeks and feeling massive
So was I right to fear the induction?
It seems the answer to that is no.
A 2014 study showed that being induced doesn’t increase the likelihood of having a caesarean. In fact women who were induced at term or when overdue were 12% LESS likely to have a C section than those who hung on for nature to do her thing. Their babies were also less likely to be stillborn or admitted to the NICU.
But can we believe this study?
We often see piles of scientific “evidence” that contradict each other. One minute coffee causes cancer the next it cures it etc. etc. so how reliable is this publication, given that it goes so strongly against the generally accepted view?
In this case the authors of the paper didn’t set up their own experiment or trial. Instead they did what is known as a meta-analysis. This is important because a meta-analysis is far more reliable than most of the scientific studies that make it into the media. The authors took the data from 157 different trials and did some serious number crunching. Looking not just at the results of those trials but at their weaknesses too. For example, many of the individual trials were pretty small, meaning their results are less reliable than bigger studies. Others were quite old or asked slightly different questions to the rest. But this variation is the whole point of a meta-analysis. By putting it all together it’s possible to overcome many of the errors and biases that inevitably influence the results of individual studies and to find a more reliable consensus.
We rarely get perfect answers in anything associated with biology. For obvious ethical and practical reasons we can’t do loads of enormous, randomly controlled trials to answer questions about human childbirth. So a meta-analysis, although still imperfect, is about as good as it gets.
But how can it be true when it contradicts so many people’s experiences?
This is the really tricky part. These results fly in the face of something many of us have learned to be true: In the experience of many women, midwives, etc. inductions tend to end in C sections. As yet I don’t know of any scientific studies to explain this difference, but if we step away from numbers and statistics for a moment, there are a few, very human, possibilities:
Relying on personal experiences is tricky. We’re all inclined to notice and trust things that confirm our existing beliefs. That’s just human nature, and it happens to everyone (I’ve known a few, usually logical, scientists get carried away over flimsy results that fit their current theory). In this case perhaps midwives and doctors who expect inductions to end in c sections are just a little more likely to remember the ones that do. Those births may also stick in the mind more than the less eventful, straight forward ones.
A similar thing can also happen with women’s own experiences. Even with everything seemingly perfect, births don’t always go to plan. Difficult births happen and sometimes they happen after an induction. If a woman has heard many times that inductions cause c sections, then it’s only natural to assume the induction was to blame if she does end up in theatre. Maybe that was the cause, but there is no way to be completely sure that the same things wouldn’t have happened with a spontaneous labour.
There is also the risk of self-fulfilling prophecies. It’s possible that some women are ending up in theatre just a little earlier than they need to because they, or those caring for them, suspected it was inevitable. Perhaps most importantly, there is the issue of fear. It is thought that fear can be a big cause of problems in childbirth. If a women is induced, and terrified of the procedure and what she’s been told it will lead to, then it could be the fear itself which causes the problems.
So should every woman be induced at full term?
What this study doesn’t do is prove that all women should be induced the second they hit 40 weeks.
There are many reasons why a woman may decide to delay or refuse an induction. I went into labour naturally but still ended up having some of the interventions that can be used in an induction and I found them pretty unpleasant. Every woman and every birth is different and each comes with a unique set of considerations. Meta-analysis and big data sets give us a clearer and more objective view of the big picture but they can’t say what is right or wrong for any individual mother. That choice must be hers and to make it women need good, evidence based information and often help from skilled, knowledgeable, health care professionals.
This paper also doesn’t give us is a very clear picture of just how likely it is that an individual induction will prevent a c section, still birth or NICU admission. What I hope we will see in the future is more user friendly data. Every women will have their own tipping point for where the numbers add up to choosing induction.
Looking pretty rough after a labour that started naturally, but still ended in an emergency caesarean
So what now?
Like many pregnant women I was taught to fear induction of labour and the cascade of interventions it would cause. Now it seems that fear was based on a myth. So it’s important that the evidence, challenging though it may feel, gets out to pregnant women and to those giving them advice. Unnecessary fear in childbirth is potentially harmful and certainly unfair. All the more so for those women who feel they have little choice but to be induced for urgent medical reasons.
This study also has implication beyond individual decisions. There is often a binary division of births. On one side the “low risk”, “normal” births that can be handled entirely by midwives and on the other “high risk” births, which are, effectively, everything else. Being induced can push an otherwise low risk woman over that line.
In the hospital where I gave birth this made a big difference. The Midwife led unit didn’t just have lower all round intervention rates, it also housed built in birthing pools and lovely en-suite rooms where mum, dad and baby could recover together after the birth. If I’d been induced I wouldn’t have been allowed on this unit. So, in choosing weather to be induced or not, I wasn’t just weighing up the risks of induction v continued pregnancy. I was also deciding if I should risk higher intervention rates, sacrifice the more welcoming facilities and deny my husband the opportunity to share the first precious hours of his child’s life. Now we have strong evidence that induction can reduce C section rates and in some cases save lives, should it really be the determining factor in where some women can give birth? Or in the standard of care they receive?
For me, spontaneous labour didn’t prevent an emergency C section. Perhaps I’d have stayed out of surgery if I had been induced? I doubt it, although I’ll never know for sure. But I can be glad that when other new mums are overdue, concerned about their baby’s health or just hot, heavy and sick of being pregnant, the myth of induction-cascade-caesarean section will be one less thing to fear.
There has been much discussion recently about safety within maternity services including a discussion on #MatExp Facebook group. A particular issue that bothers me is the idea that safety and experience might be two separate and mutually exclusive issues and it is this thought that drives me to write today.
Safety is paramount. The purpose of maternity services is to provide safe care through the journey of pregnancy and early newborn life. Every appointment in the NICE pathway is designed to screen for potential problems and ensure they are managed effectively. Every healthcare worker know this is the aim. The 20 week ‘anomaly’ scan might be considered the time to discover the sex of your baby if you wish and to get some photos but the medical purpose is to ensure the baby is growing well, with no abnormalities and to check where the placenta is localised to exclude placenta praevia (low lying placenta) which can cause life threatening bleeding.
But there is more to pregnancy and becoming a parent than safety isn’t there? I am currently reading Atul Gawande ‘Being Mortal’ where he eloquently demonstrates that keeping elderly people ‘safe’ is not enough, there is more to life and living than safety alone. He describes a number of times when giving elderly people purpose such as a plant or animal to look after or more freedom to live the way they wish despite disability it makes a significant difference to their wellbeing. Sometimes this path may deemed ‘less safe’ but for that individual may make all the difference. This comes back to choice. Safety & choice can be tricky ones to combine successfully.
This does not mean I am belittling safety. As a consultant obstetrician it falls to me to talk to couples when the worst has happened and their baby has died. I also care for women who have had unexpectedly life threatening complications. I know I am with them during probably some of the darkest hours they will ever experience. I cannot pretend to understand how they feel but I do know I have been part of those intimate moments of grief and with some families that has followed through into supporting them sometimes for years. As a hospital we have a robust process of incident reporting and the feedback from a Serious Incident investigation (SI) again will sometimes fall to me. In some cases there is nothing that we think could have been done differently in some cases I have to sit and tell an anguished couple that we have failed them and that maybe things could have been different. It is a devastating thing to do, there is absolutely nothing that can be said that will make the situation better. It feels as if you have personally taken their existing despair and dragged them into an even more unthinkable place and the only thing you can say is ‘sorry’ which feel hopelessly inadequate and trite for such a situation.
So if I could guarantee safety I would in a flash but it is not that simple. Maternity care is delivered by people and unfortunately to err is human. We cannot design a system free of risk because however hard we try the variable of human error gets in the way. We can introduce systems that help minimise the impact of these errors but we can’t eliminate them. My favourite analogy for risk management is James Reason’s model of Swiss cheese. The event only happens when the holes in the ‘cheese’ line up the rest of the time the barriers put in place prevent the error. An example in maternity care might be the introduction of what we call ‘fresh eyes’. A midwife looking after a woman on electronic fetal heart monitoring might misinterpret this or not see the subtle changes over time if she has it in front of her constantly. ‘Fresh eyes’ means another midwife or obstetrician comes and looks at the trace on an hourly basis. This means if unusually the first midwife has made an error there is a system that means it is more likely to be corrected.
The concept of a ‘No Blame’ culture is another example designed to minimise human error. The idea that if one sees or makes an error one should report it without fear so that learning can be gained from it. It may be the learning will be the need for some individual training but equally it might be something totally different. If staff are fearful of consequences then under reporting might be the result and safety gaps may not be identified. Encouraging openness about mistakes and errors is vital but difficult. In maternity it isn’t as if we can just operate our way out of this problem .We know the huge rise in Caesareans sections in the last 30 years has not improved the outcomes for babies but has instead cause maternal health problems. So in maternity as other medical specialties we have to constantly refresh and re-invent what we are doing to try and improve safety. As obstetricians we tread a difficult path trying constantly to call correctly just the right amount of intervention at just the right time.
So where does experience fit in I hear you ask? There is abundant published evidence of positive association of patient experience with clinical safety and effectiveness, in other words if your patients (or I prefer users) are having positive experiences then you are running a safer service. It’s hardly surprising if we communicate and explain things to women and their families that we will be more likely to communicate effectively to other members of the multidisciplinary team. If we are open and honest then woman can challenge assumptions and make sure we haven’t missed something critical, a woman knows her own history inside out whereas we might omit a key point. To me one of the most shocking things that was said at our ‘Whose shoes’ #MatExp workshop last year was that women can feel intimidated and unable to ask questions. Trust and understanding between health professionals and those we care for are vital. We cannot possibly hope to improve safety in isolation, experience has to improve too.
There are two specific elements of #MatExp of which I think epitomise the safety -experience overlap. The first is an on-going ever growing constructive conversation between women, families, obstetricians, midwives, health visitors, paediatricians, families and anyone involved in maternity services. Only by tackling the difficult conversations without hierarchy in an equal and respectful way can we improve maternity care. Listening and talking to one another is critical not only as we work with women but in dissolving those barriers and difficulties that sometime exist between different professionals. Flattening of hierarchy, team work and the ability of anyone to challenge is a well-recognised component of a safety culture. We are doing this both locally using the workshops and board game and more broadly via social media and the website.
The second element of #MatExp is that personal sense of responsibility to take action. Own what you are doing and why you are doing it. ‘Wrong is wrong even if everyone is doing it’ that doesn’t mean leave it to someone else. It means that health professionals and women can take action and influence maternity experience up and down the country and through that impact on and improve the safety of maternity care. So in final answer to my question I do not think it is a choice safety or experience I believe the two are fundamentally intertwined. So what will you do to improve #MatExp?