It’s nearly a week since lighting the fuse and setting off #FlamingJune with a bang. We launched our website and we are starting to see that ripple of action as a result as well as trying to draw on existing events and plans that we knew were happening in June.
It is getting people’s attention – perfect, just as we hoped! We are being quoted and used as an example, as a change platform, a campaign it’s awesome!
But in some ways we are victims of our own success we are just that bit too innovative and cutting edge so it is hard for people to understand just what we are.
We are not an organisation, we are not employed to do this, we have no funding, we have no rules or structure.
We are quite simply people. People who are like minded, people with initiative, people who see the need for change and want to enable it to happen by bring ideas together and encouraging action.
Some of us it is true are NHS employees however this work is not in our job description we are doing this in our spare time round busy day jobs and home life. Many of us are juggling this with other jobs, small children, home commitments, life… the thing that unites us is a passion and an energy to keep improving maternity services.
So if I were to define us, we are an ever growing fluid and flexible movement of people who want to enable change and improvement in maternity services.
There are no rights or wrongs, no one needs permission to join in, we are leading by default because we happened to step forward.
There is plenty more space for people to step in to help. The key message is to value and respect all views; encourage airing problems to find solutions and we will endeavour to help and support those who can and want to jump on board as best we can.
We have a lot of exciting days to come in June & beyond. Bring it on!
There have been some fantastic conversations taking place on the MatExp Facebook group, with a new ACTION thread every day to generate discussion. The aim of these discussions is to identify ways that we can ACT to improve maternity experiences. Big, long-term actions that might require system change or a change in culture. And small, immediate actions, that professionals and individuals can take today to improve the maternity experience of those around them.
One of the first topics we looked at was Anxiety, as it had been one of the first issues raised on the MatExp ABC.
“Anxiety” covers a number of areas when we look at maternity experience. Mothers can have existing problems with anxiety, that have already been identified. They could have had anxiety for some time but the experience of having a baby has intensified it (my experience). It could be that they begin to suffer with anxiety postnatally – Emma Jane Sasaru has written here of her experience of perinatal anxiety. Or perhaps their anxiety is focused on giving birth – many mothers are incredibly anxious about what the end of pregnancy has in store for them. Finally, there will be mothers who have experienced birth trauma or baby loss and this can understandably provide a background for anxiety in subsequent pregnancies.
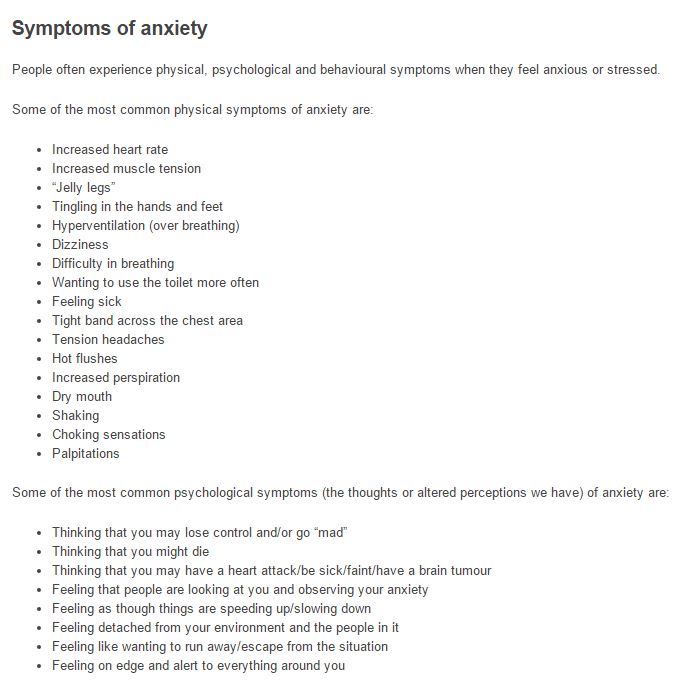
Anxiety UK says of anxiety that it is “something that can persist whether or not the cause is clear to the sufferer”. The organisation lists the symptoms as
Anxiety UK Registered Charity Number (1113403) Established 1970
Certainly, on a personal note, “feeling detached from your environment and the people in it” goes some way to explaining why it took me such a long time to properly “fall in love” with my babies. There was no “rush of love” for me when I gave birth and first held my children, despite my having positive birth experiences both times. “Feeling like wanting to run away / escape from the situation” – many new mums feel like this at times when coping with a newborn baby but it is important to recognise when feeling like this “now and again” has accumulated into something more problematic.
So how can we ACT when anxiety is a factor in maternity experience? Let us first look at how women can help themselves:
Practice HYPNOBIRTHING – a number of people involved in the #MatExp campaign suggested this as a great way to alleviate anxiety in pregnancy and anxiety about birth itself. Pregnancy Coach Suzy Ashworth explains here what hypnobirthing is all about, and how it’s beneficial for all women regardless of the way they plan to give birth.
BE HONEST and try to explain your anxieties to your healthcare professionals. Find out as much as you can about anxiety and ways to manage it.
Now these actions all assume that the woman in question is aware that she is struggling with anxiety. But this is certainly not always the case. This is where the birth professionals come in. How can they act when anxiety is a factor?
Understand how anxiety can manifest itself. If a women is finding it difficult to talk about something, if she is quiet and refusing to engage with a situation, if she practices avoidance by walking out on a conversation then think “anxiety”.
Give women the opportunity to talk openly about their fears, and really LISTEN.
Offering reassurance can be helpful but it can also be dismissive – being told “don’t worry, that won’t happen” can heighten a woman’s anxiety as she will feel as though her fears are not being taken seriously. Always remember that those fears are REAL to her, however bizarre they may seem to you
What services are available to women in your area who are struggling with anxiety? Are the following available (and do you know how to access them?) or do they need to be put in place?
Hypnobirthing, mindfulness and meditation classes
Cognitive Behavioural Therapy (CBT)
Specialist mental health midwifery teams
Training for midwives and health visitors on recognising anxiety
Where services are available, there are simple ways in which women’s access to them could be improved:
Please check on the mental health of the women you care for throughout their pregnancy and postnatal period, not just at their booking in appointment.
If you offer anxiety support, please make it possible for women to enquire about these services by email, not just by phone. Phone conversations are very difficult for many anxious people, and services only being accessible by initial phone assessment put up a real barrier.
When we look specifically at prenatal anxiety, there are changes to our birth culture that could make a big difference:
Empower women to trust their bodies. Too many women fear that they will not be able to give birth safely – how can we help them to understand how their body works and reacts in labour, and how it can be supported and encouraged to do its job?
Ensure that women understand that they have the control to make their own birth choices. Feeling as though they have no control is a huge factor for anxious people, but encouraging informed choice and putting women at the centre of their birth experience can help to alleviate this.
As with almost every discussion of maternity experience, continuity of care becomes an issue. Where women know their birth professionals and have built up a relationship with them, anxieties are reduced. Whilst continuity of carer is offered in places on the NHS this is far from the norm at this moment in time. If you struggle with anxiety then there are care options available to you to ensure that you have continuity in pregnancy and beyond:
Use an independent midwife. There is a cost involved in engaging the services of these professionals, but it is always worth speaking to them before dismissing the idea on the basis of cost, as there may be ways that the cost can be reduced.
Use a OnetoOne midwife. This is a “free at the point of delivery” service, but unfortunately it is only available in some areas. Find out if they are commissioned near you.
Use a doula. Doulas support women and their families during pregnancy, childbirth and early parenthood. This support is practical and emotional but non-medical in nature. Again, there is a cost involved, but there are ways that this can be reduced so it is worth contacting your nearest doulas to discuss the options open to you.
Lindsey Middlemiss (aka “Newbury Doula”) is having lots of discussions at the moment about the wider provision of doula support for women with high anxiety of at high risk of PND, including women who have experienced baby loss or who have had birth trauma. There is a possibility of some NHS funded pilots and research studies in the future, and the Doula UK Access Fund will likely be changing and expanding its criteria. We eagerly await developments in this regard.
#MatExp “Language” Champion Leigh Kendall has written extensively about support for bereaved parents and I know she will be suggesting further actions during #FlamingJune. Therefore I don’t want to focus too much here on anxiety in those who have experienced loss, but one thing did come out loud and clear from the discussions we had on Facebook:
There is currently no standard care pathway for those who are pregnant following the loss of their baby. They might be labelled “high risk” depending on whether baby loss was a result of pregnancy complications, but their emotional needs are not automatically met.
This is staggering to me.
This has to change.
On a positive note, one member of our community is aware of midwives at her local hospital looking into setting up Rainbow Antenatal Clinics specifically for those who are pregnant following loss. Is this something that you could look into at your hospital? Is this something you already offer?
Another positive that I would like to finish on is the new provision of antenatal appointments from our health visiting teams. Vanessa (aka Frustrated HV) had this to say on the subject, with specific reference to pregnancy following loss:
“I really do hope that the antenatal visiting programme being undertaken by health visitors & the increased communication between midwives & health visitors & GPs will mean that fewer women experience this neglect… Because it has to! A known history of loss in or around pregnancy should now automatically trigger (through midwife reporting) a Universal Plus antenatal health visiting service. Which would mean that you would have support throughout the pregnancy (as well as after) & signposting/referral to more specialist services if needed. No one should still be experiencing this type of trauma. You are correct that lots still needs to be done, but lines of communication are being created & general awareness is improving & I know that with the continued efforts of all the people I have seen in #MatExp& through all the conversations & wisdom shown, we will change things for the better.”
June is our month of ACTION for the #MatExp campaign! All actions big and small are welcome and very valued.
Actions don’t need to be huge or onerous. They could be something you’re already doing. For example, my action focuses on bereavement support for parents who have lost a baby. It is an extension of my blog, and the work I am already doing as part of Hugo’s Legacy.
Your action could be as straightforward as telling everyone you know about #MatExp, and encouraging them to get involved.
If you’re a health professional, it could be something as simple as making sure you always say #hellomynameis. Or, your action could be doing something differently based on feedback from a woman in one of the #MatExp social media channels.
It doesn’t really matter what your action is. Your action should just be something that is relevant to YOU. It should also be something that feels manageable and achievable.
We all have busy lives. Like with any change, to be sustainable it needs to be part of your life, not in addition to it.
You may have seen some comments from folk saying they want to do more, and that’s brilliant. But please remember that is pressure they are putting on THEMSELVES. We think it would be brilliant if everyone made an action, but there is no pressure from us.
There is also no pressure to do the action during June. #MatExp has already achieved so much, and generated so much activity since its official launch at NHS Change Day in March 2015, we have designated want to maintain the momentum. Dependent on your chosen action, it might be something you will do every day, or it might be something it is difficult to put into action for some time yet. Throwing a few clichés around, Rome wasn’t built in a day, and remember how you eat an elephant: in small chunks!
#MatExp is a grassroots movement – that is, it’s led by us all. No one is ‘in charge’ as such. That means you don’t need to ask anyone for permission to do an action (caveat: dependent on your action, of course: you might want to get permission from someone in your organisation if your action involves something like moving a ward!).
Do share with the #MatExp community what your actions are, or about the actions you’re thinking of making, though. That’s not just because we’re a nosey bunch: by sharing our thoughts, we can collaborate by contributing different ideas from our own experiences and expertise. By doing that we can help each other out, and potentially make an even greater impact.
We have seen from our discussions on Twitter and in the Facebook group that discussions around actions create all sorts of lightbulb and penny drop moments.
You can:
Tweet using the #MatExp hashtag
Join or start a conversation in the #MatExp Facebook group
If you have a blog, you could write a post about the action you are thinking of making, or have made, and add it to our linky
If you don’t have a blog, you can tell us about your existing or proposed action through this contact form
You can also share your action by taking an action selfie and sharing it on social media. There is a template you can print out on this page.
Here’s my selfie!
Together we are stronger.
There are no right or wrong answers!
Don’t worry if your action seems ‘too small’. No action can be too small. There are no points to be scored, no prizes to be given – and that’s not just because this campaign is run on zero budget – scores are not what #MatExp is about. Making an action that impacts on even one person is amazing, valued, and very worthwhile.
You may have heard of the starfish story:
We hope that makes sense. If you need any guidance or would like to do some brainstorming or have ideas you’d like to share, please do throw it out to the #MatExp community – on Twitter, Facebook, or by looking at some of the ideas on this site. The principle that underpins #MatExp is identifying and sharing best practice across the nation’s maternity services.
There is no false modesty involved when we say we are making it up as we go along – we really are. And that means YOU can help influence the directions #MatExp takes.
It was on 12th May that Leigh Kendall and Helen Calvert thought about starting a Facebook group for the #MatExp campaign. JFDI and all that, the group was started two days later. Three weeks in and we’re at 450 members. You’ve got to love this campaign, nothing happens slowly!
The group is administrated by Emma Jane Sasaru, Helen Calvert,Leigh Kendall and Susanne Remic, and is the Facebook outlet for a campaign that has already gained huge momentum on Twitter. Florence Wilcock, the obstetrician at Kingston Hospital who started the campaign, has always wanted it to be focused on ACTION and this theme is central to the group. Each day a member of the admin team starts a thread on a chosen topic with questions/talking points and a request for actions that families and birth professionals can take to improve maternity experience in this area. We ask that actions are S.M.A.R.T.
Florence and Gill Phillips have a Month of Action planned for June, so we had originally hoped to do a blog post at the start of June detailing the actions put forward so far by the Facebook group and asking that people get involved. The snag is there have been so many fabulous actions put forward already on a number of important topics. The topics are being chosen in alphabetical order as a nod towards the #MatExp ABC that provided so much impetus on Twitter, and we are so far only on “H”– already the actions are numerous and thought provoking.
So we have quickly realised that it might be better for each of the admin team members to do individual blog posts on the topics that they have introduced to the group. These posts will start to come through soon, but for now we still wanted to give you a flavour of the suggestions and we hope that you will join us on Facebook or Twitter (or both) to get involved.
ACTION!
The actions that have been suggested on each of the threads can be divided into two categories:
Immediate – just get up and do it actions that anybody can take, here and now. These tend to be small things but they can still have an impact.
Long-term – group actions that require input and buy-in from different places and will probably require campaigns of their own.
Both are very important to the campaign. There are big issues that need to be addressed in maternity care and the NHS Maternity Review is looking at these right now. We are hoping to work with the review panel and to share our ideas with them. But we also need to remember that simple acts of kindness can change the experience of anyone with whom we come into contact. Sharing a piece of information could send someone down a different path. Signposting to a service could make the difference for that individual. No one needs to sit back and wait for a bandwagon to jump on. We can all of us get up and act today.
So what has been suggested so far? Here is a snapshot of some of the topics we have discussed:
A is for Anxiety
Immediate actions –
Anxious mums to use hypnotherapy techniques in pregnancy
Be honest about your anxieties and find out as much as you can on how to manage them
Midwives please ask mums about their mental health throughout their pregnancy, not just on booking in; anxious mums to look into mindfulness techniques
Long-term actions –
All health visitors need training in identifying and supporting pre and postnatal anxiety
Subsidised doula provision for anxious families
Continuity of care for anxious families
Refer anxiety sufferers to specialist mental health support
B is for Bereavement
Immediate actions –
The most important immediate action can be done by anyone, anywhere, anytime – acknowledge the baby the parents have lost. If you know the baby’s name, use it. If you don’t know the baby’s name, ask. Take the parents’ lead on whether or not they want to talk about their loss. Try not to worry about saying the ‘wrong’ thing. The worst thing you can do is to skirt around the subject, or ignore it completely. To do so insulting and upsetting to bereaved parents.
Long-term actions –
Clear, concise, sensible, and up-to-date information to be provided to bereaved parents when they leave the hospital after the death of their baby. Parents need reassurance about the emotions they are likely to feel, and a few pointers about how to navigate grief, especially during the raw early weeks. The information also needs to clearly state how the parents can access appropriate support as and when they are ready.
Access to counselling support. Too many bereaved parents have had to fight for the counselling and psychological support they need – or have gone without. Some hospitals do offer counselling services: hospitals need to make clear to parents that this is available, and how to access it. Funding issues mean that not every area is able to provide these services, but charities thankfully do exist to fill the gap. Hospital and GP practice staff need to know what support is available locally so they can signpost parents appropriately, or where appropriate make referrals for them. Leaving bereaved parents to source their own support at a time when they are least able to have the tenacity to deal with ‘the system’ is unacceptable.
Training in bereavement care for health professionals. Surprisingly, many don’t receive this as standard practice. The vast majority of health professionals are caring individuals, but a lack of appropriate training means many are unsure about how best to deal with bereavement, which may lead them to saying things that are less than helpful to parents. What is said to parents at this sad time stays with them forever, so the importance of this training cannot be underestimated. This training should be extended to all staff involved with maternity/NNUs (including admin, housekeeping et al) to help prevent unnecessary upsets.
Debrief/support to care for the needs of maternity, obstetric and NNU staff after the death of a baby. These staff are deeply affected by the loss of a baby in their care.
B is for Birth Trauma (families)
Immediate actions –
Use of language when discussing birth trauma with families- lots of women have felt their feelings were dismissed, or that they were being ‘silly’. Women also felt that they had failed. Language in notes also very important.
Immediate debrief after a traumatic birth; women felt that they were discharged and sent home without having the chance to talk through events.
Communication- tell women and their families what is happening and why.
Long-term actions –
Birth trauma support groups for women to access after a traumatic birth.
Birth reflections and birth trauma counsellors to be accessed for as long as women and their families need them. Trained counsellors to support, and health visitors to be able to signpost the necessary services too.
Better recognition of PTSD following birth trauma and better support for dads too.
Emotional support for women in subsequent pregnancies.
Ensure that women know how to access appropriate services following birth trauma.
B is for Birth Trauma (midwives)
Immediate actions –
Make sure your colleagues know that they don’t have to “cope” – it’s okay to admit that they have been traumatised by a particular birth experience
Ask if your Trust has guidelines in place for supporting staff after a difficult birth.
Long-term actions –
Stringent debrief sessions put in place for each instrumental birth and any birth that is not straightforward
Tackle trauma that accumulates from seeing the same things again and again – e.g. vaginal exams with inadequate consent, instrumental deliveries without compassion, loss of autonomy and consent.
C is for C-sections
Immediate actions –
Skin to skin in theatre.
Ensure that women are supported in their decision to have a c-section and help them to write a birth plan to feel empowered during surgery. Discussion of gentle c-section options.
Help women to find comfortable positions to breastfeed.
Long-term actions –
Identify reasons for c-sections and look to see where these can be reduced.
Educate women during subsequent pregnancies, ensuring that up to date information is given with regards to VBAC. Ensure access to VBAC clinic is given.
Better patient leaflets with more information on what happens during surgery and what recovery is like.
Debrief from surgeon on how the c-section went and how subsequent pregnancies are likely to be affected.
Better support for women after an emergency c-section.
Provide emotional support and/ or counselling after a c-section for women who require it.
C is for Complications
Immediate actions –
Communication was a common theme in the responses in this thread. Women – especially those who experienced complications around the time of the birth of their baby – wanted professionals to explain what was happening. Not knowing what was happening, and why, added to these women’s anxiety. Women (and their birth partners) need to be told as much as is appropriate at the time what is happening and why, in simple language.
Health professionals need to remember that consent is still vital!
Explain everything – as a health professional, certain things that you consider routine may be daunting or scary to a woman in your care. Make sure you explain everything that is happening, and be patient if they need the information to be repeated – it can often be difficult to take things in when you are in a crisis situation.
Long-term actions –
Information: there is a lot of difference in the quality and content of information pregnant women receive from hospitals and community midwives. It can create confusion, especially combined with the wealth of information available from charities and the internet. While the internet can’t be controlled of course, it would make sense for hospitals nationwide to have consistent leaflets from a central source, with the ability to personalise information as appropriate.
Connected to this point, knowing how much information to tell women about complications is difficult. We want them to know enough so they can recognise symptoms if they appear, but not so much they are stressed and scared. The balance is hard to strike. To compound this, there are women who do not attend antenatal appointments so are unable to receive this information.
For A&E staff to be better aware of pregnancy complications, and to consult maternity/obstetrics staff when needed.
For women to be proactively contacted when pathology (blood/urine etc) tests come back with warning signs, rather than relying on the woman to remember to phone for results.
C is for Continuity of Care
Immediate actions –
Managers to talk to the independent midwives and social enterprise midwives who are knowledgeable in how case-loading can work
Look at the Streatham Valley midwifery team in London for a working model
If a woman is not receiving continuity of care, please ensure as a birth professional that you read her notes thoroughly and write good notes for the next person she sees.
Long-term actions –
We need strong leaders at the helm of Trusts who understand how to lead midwives towards the implementation of continuity of care