As we reach the middle of #FlamingJune I have been thinking about the week I’ve had. To be honest it has pushed my multitasking abilities to the limit: I have had a number of big events to attend or speak at, as well as the day job of being a divisional director at Kingston and a clinician seeing and caring for women – and this is before I even consider my husband and daughters.
Amongst all this I sometime wonder if #MatExp is really having an impact, or have I just got carried away.
It has been a tricky week for others too. The more people know about #MatExp and what we are trying to do the better, but this comes with pressure and also criticism.
It is hard to understand that this is an organic grassroots project with a direction and mind of its own. No one is ‘in charge’ and it is richer for it.
This was brought home to me at the London Maternity Strategic Clinical Network event held on Wednesday. The five pilot sites who had held a #MatExp ‘Whose Shoes’ workshop presented the action they had taken as a result and I was overwhelmed by the diversity of actions taken and the determination with which people had followed through in a multitude of ways.
Devolved leadership and true collaboration with women has been our hallmark from the beginning but I was bowled over to actually witness the results of all the actions gathered together in one place and to recognise how powerful the outcome of the workshops was.
At the same event we launched our ‘Maternity Experience’ film. It was a tense moment, it is so difficult when you are knee-deep in a project to step back and see it afresh and I wasn’t sure how others would find it. I so desperately wanted it to to be true to the workshops and #MatExp conversations we have had over the months.
Fortunately on the whole it seems to have rung true and be a success, which I hope will power more thinking and questioning on a daily basis of ‘why do we do it this way, what could we do instead?’
Rounding off my week I have had the small matter of conversations with the leadership of the Royal College of Obstetricians and Gynaecologists (RCOG) about how they could help, and a flying visit by Helen Bevan to Kingston on Thursday when she said ‘there was lots going on #MatExp yesterday, I got tweeted your film about 15 times!’.
It’s a roller coaster ride but I wouldn’t have it any other way. Each time I have a doubt something happens that reaffirms that however small , changes are actually happening. Just yesterday a midwife at Kingston told me her pledge from our October workshop will be completed next week. She has stuck with it through barriers and blocks and seen it to completion and that desire for action, that is what #MatExp is all about!
It’s nearly a week since lighting the fuse and setting off #FlamingJune with a bang. We launched our website and we are starting to see that ripple of action as a result as well as trying to draw on existing events and plans that we knew were happening in June.
It is getting people’s attention – perfect, just as we hoped! We are being quoted and used as an example, as a change platform, a campaign it’s awesome!
But in some ways we are victims of our own success we are just that bit too innovative and cutting edge so it is hard for people to understand just what we are.
We are not an organisation, we are not employed to do this, we have no funding, we have no rules or structure.
We are quite simply people. People who are like minded, people with initiative, people who see the need for change and want to enable it to happen by bring ideas together and encouraging action.
Some of us it is true are NHS employees however this work is not in our job description we are doing this in our spare time round busy day jobs and home life. Many of us are juggling this with other jobs, small children, home commitments, life… the thing that unites us is a passion and an energy to keep improving maternity services.
So if I were to define us, we are an ever growing fluid and flexible movement of people who want to enable change and improvement in maternity services.
There are no rights or wrongs, no one needs permission to join in, we are leading by default because we happened to step forward.
There is plenty more space for people to step in to help. The key message is to value and respect all views; encourage airing problems to find solutions and we will endeavour to help and support those who can and want to jump on board as best we can.
We have a lot of exciting days to come in June & beyond. Bring it on!
June is our month of ACTION for the #MatExp campaign! All actions big and small are welcome and very valued.
Actions don’t need to be huge or onerous. They could be something you’re already doing. For example, my action focuses on bereavement support for parents who have lost a baby. It is an extension of my blog, and the work I am already doing as part of Hugo’s Legacy.
Your action could be as straightforward as telling everyone you know about #MatExp, and encouraging them to get involved.
If you’re a health professional, it could be something as simple as making sure you always say #hellomynameis. Or, your action could be doing something differently based on feedback from a woman in one of the #MatExp social media channels.
It doesn’t really matter what your action is. Your action should just be something that is relevant to YOU. It should also be something that feels manageable and achievable.
We all have busy lives. Like with any change, to be sustainable it needs to be part of your life, not in addition to it.
You may have seen some comments from folk saying they want to do more, and that’s brilliant. But please remember that is pressure they are putting on THEMSELVES. We think it would be brilliant if everyone made an action, but there is no pressure from us.
There is also no pressure to do the action during June. #MatExp has already achieved so much, and generated so much activity since its official launch at NHS Change Day in March 2015, we have designated want to maintain the momentum. Dependent on your chosen action, it might be something you will do every day, or it might be something it is difficult to put into action for some time yet. Throwing a few clichés around, Rome wasn’t built in a day, and remember how you eat an elephant: in small chunks!
#MatExp is a grassroots movement – that is, it’s led by us all. No one is ‘in charge’ as such. That means you don’t need to ask anyone for permission to do an action (caveat: dependent on your action, of course: you might want to get permission from someone in your organisation if your action involves something like moving a ward!).
Do share with the #MatExp community what your actions are, or about the actions you’re thinking of making, though. That’s not just because we’re a nosey bunch: by sharing our thoughts, we can collaborate by contributing different ideas from our own experiences and expertise. By doing that we can help each other out, and potentially make an even greater impact.
We have seen from our discussions on Twitter and in the Facebook group that discussions around actions create all sorts of lightbulb and penny drop moments.
You can:
Tweet using the #MatExp hashtag
Join or start a conversation in the #MatExp Facebook group
If you have a blog, you could write a post about the action you are thinking of making, or have made, and add it to our linky
If you don’t have a blog, you can tell us about your existing or proposed action through this contact form
You can also share your action by taking an action selfie and sharing it on social media. There is a template you can print out on this page.
Here’s my selfie!
Together we are stronger.
There are no right or wrong answers!
Don’t worry if your action seems ‘too small’. No action can be too small. There are no points to be scored, no prizes to be given – and that’s not just because this campaign is run on zero budget – scores are not what #MatExp is about. Making an action that impacts on even one person is amazing, valued, and very worthwhile.
You may have heard of the starfish story:
We hope that makes sense. If you need any guidance or would like to do some brainstorming or have ideas you’d like to share, please do throw it out to the #MatExp community – on Twitter, Facebook, or by looking at some of the ideas on this site. The principle that underpins #MatExp is identifying and sharing best practice across the nation’s maternity services.
There is no false modesty involved when we say we are making it up as we go along – we really are. And that means YOU can help influence the directions #MatExp takes.
#FabObs Florence Wilcock ensured that her roles as obstetrician and mother blurred a bit more (and took many of her colleagues by surprise) when she did something truly wonderful in terms of making people think, really think about the experience of the women they are caring for. She walked in their shoes, which on this occasion involved taking off her shoes…
Flo’s pledge
It is brilliant that Flo has taken the time and trouble to reflect in such detail and share the learning…
Florence Wilcock writes: For NHS change day I wanted something that made a statement that said “#MatExp has arrived, take notice, we are improving maternity experience, get involved!” I couldn’t quite think of the right action until I saw a twitter exchange with Damian Roland back in December and watched a video where he described his spinal board challenge from NHS Change day, 2014. I had a light bulb moment thinking what would be the maternity equivalent? Lithotomy!
Lithotomy is when we put a woman’s legs up in stirrup; sometimes this can be essential for an assisted birth with forceps or ventouse (suction cup) or if stitching is required. But sometimes we use lithotomy position for normal birth or when stitches are minimal. In our #MatExp Whose Shoes? workshops, my favourite card is one based on Gill Phillips’ Mum (now aged 93) being made to take castor oil, despite telling the midwife it would make her sick. And it did. The card asks what is common practice now that will similarly seem wrong or odd in the future: the unanimous answer given at Kingston was lithotomy.
I started to think about whether we use lithotomy more than we should and wondered what does it feel like? Although I have two daughters, they were both born by emergency Caesarean so I do not have personal experience of lithotomy although I know some of my midwifery and consultant colleagues already do. It seemed the perfect challenge. I chose to do try it for one hour as that is a quite realistic time that a woman might be in that position, sometimes it can be less, but sometimes it can be far longer.
I decided to wear a hospital gown and some running shorts as it didn’t feel quite right to do it in normal clothes. The first thing I learnt was that the hospital gown was stiff and itchy, I couldn’t get it to do up properly without assistance and when I had finally tied it I sat down to discover it felt as if I was being strangled by the neck line so had to loosen it off immediately. I adjusted the back of the bed but found it quite hard to swivel round & reach the buttons to do so. We put on a fetal heart monitor which just felt like a normal waistband, a blood pressure cuff and stuck an IV line on my arm. We also used a doll to give me a bump. I know not all women will have all these attachments but many will. During this time Tom, who was going to follow me with the challenge, commented that I looked anxious from my body language before I had even begun and it was true I felt quite apprehensive with all these people running around being aware I was about to be totally in their power as it were.
We were finally ready for ‘legs up’! The first thing I discovered with a slight shock was that the stirrups were very cold which I hadn’t expected at all. The other observation was that the people started adjusting my legs without asking me. I thought one leg was going to fall off as the stirrup wasn’t tightly fixed enough and I was in a slightly twisted position which I asked them to adjust. Once that was done I felt reasonably comfortable and relaxed. They took my blood pressure with an automated cuff which was surprisingly painful. I decided to have a breech baby and we took a few photos.
Twenty five minutes in we decided it was time to take the bottom of the bed off which we would do for an assisted birth. I felt immediately more precariously positioned and vulnerable like I might fall off of the bed. The midwives put my legs higher and the bed much higher off the ground which was the right position for delivery without causing them back problems. This felt quite odd to be high up in the air or as one midwife put it ‘face to vagina’ so that she could see what she was doing at eye level! I definitely could not have got down from there unaided especially not when contracting and in pain. A midwife walked into the room with the door & curtain open and I realised I could see all the way down the corridor which meant everyone in the corridor could potentially see me. Obviously this was a simulation but it did emphasise to me even more the importance of closing the door & curtain behind you to maintain privacy.
A series of people then came to talk to me. Our chief executive Kate Grimes popped in for a chat and asked if I was willing for a film crew to come in to which I agreed. By this point my bottom (sacrum) was getting pretty sore & I had neck ache. I was feeling fairly uncomfortable. My abdomen felt quite compressed and I thought if I was a woman in labour having to push it would probably make me feel quite nauseous.
I was prepared to be filmed and photographed but it was interesting that a number of people walked in and out to look without talking to me. Helen and the presenter introduced themselves to me but the camera man did not and did a series of sound checks over me and proceeded to film without even speaking to me. I am sure it was an oversight but it gave me an amazing sense of being dehumanised and re-emphasised the importance of #hellomynameis.
In the middle of this Kate Greenstock, our MSLC co-chair arrived. Kate is a doula and came straight to me and asked if I would like a foot massage. Although I thought I was fine, as soon as she asked me I realised actually that I wasn’t fine and here was a person who wasn’t laughing or making a spectacle of me but who actually cared about how I felt. That isn’t to say all the wonderful midwives didn’t but at that moment I felt like Kate and I understood one another and that this was tough and she was ‘on my side’ as it were here to support me.
She gave me a foot massage which was immediately relaxing. I have always understood the importance of support in labour but felt that women could get that from our wonderful midwives and struggled to understand why they wanted a doula too. This experience gave me some inkling of why in some situations a midwife might be focusing on other things and a doula might be able to focus on how the woman is feeling and that alone.
My hour challenge was ticking by and for a short time after the film crew the room emptied out and I was left almost alone. I felt slightly abandoned after such a crowd before and realised if the midwives didn’t come back I was rather stranded in an undignified position. It is not unusual after an assisted delivery for many people to come in and then gradually disappear leaving me as the obstetrician to suture on my own, the midwife popping in and out to get things so in a way this behaviour seemed quite apt.
The midwives returned with a nice plastic baby so that I could have #skintoskin and then my hour was up. The end of the bed was put back in place with the bed rocking as they pushed the parts together and then finally they brought my legs down and it was over.
So what was the impact of me undertaking the lithotomy challenge?
My action has certainly got others thinking and talking. I started tweeting about it in the weeks before change day and challenged a few colleagues. I’m greatly indebted to Professor Jim Thornton who was the first to accept and kicked off a whole week ahead of NHS Change Day.
I know of at least twelve others who have undertaken the challenge and five more who have promised to. The challenges are spread across 10 organisations so I am hoping for a ripple of conversations as a result. Even those that say ‘no’ learn something from asking themselves the question.
An obvious action as a result is for staff to think about trying to avoid lithotomy altogether. There are a multitude of options for positions and care in labour that we can employ. The Better Births initiative is an ideal example of a resource any midwife can access. Environment is also all important: birthing pools, stools, mats, balls are something tangible people can change. Antenatal education and preparation, both NHS and with our partners in the community, is also vital.
For us obstetricians there are certainly situations in which lithotomy is invaluable and necessary however this challenge has definitely made me think about the consequences of the length of time and how to keep it to a minimum as the position became much more uncomfortable after half an hour. Sometime in the pressure of work, helpful midwives get women ready for us in position before we enter the room and I had not given much thought to the impact of additional time or someone new entering the room when you are already in this position. The careful use of sheets or drapes to minimise exposure was also a topic for discussion.
In conclusion my hope with my challenge is that in each Trust conversations will happen that change practice and via networks and social media good practice will spread. I hope it will have the ‘butterfly effect’ where one small change in one place will result in large differences later.
Imagine, a consultant, a midwife, a doula, a support worker, a commissioner, a campaigner and a mother all coming together to help support and improve maternity services for all women and their families.
Wonderful you may say, but will this really ever happen you may wonder? The answer is yes!
#MatExp is a wonderful grassroots campaign using the Whose Shoes?® approach to help identify and help improve our national maternity services. By means of workshops in local hospitals users of maternity services are brought together with others to join conversations about their experiences of maternity care and share what really made a difference to them personally and their experience and talk about ways that care can be improved. These workshops enable health care professionals (in and beyond the NHS) and local communities to listen and work in partnership with women and their families to find ways to improve local and national maternity services. Anyone can take part whether your a maternity service user, partner, community group or NHS staff, from chief executive to volunteer all are welcome to attend and share. Also on twitter using the hashtag #Matexp there are many amazing people sharing personal stories, experiences, achievements and ways they are actively trying to improve care both in there local hospitals but nationally too.
I personally have been involved in a #Matexp campaign for NHS change day. It was action 5 – ‘life with a new baby’ as breastfeeding champion along with the lovely Helen Calvert. Personally for me #Matexp has been really wonderful and something im proud to be part of. After suffering poor care with my first birth and subsequent birth trauma and PTSD, #Matexp has given me hope.
Hope that things can change.
Hope that women will be the centre of maternity care.
Hope that the culture of birth and our maternity services will improve.
Hope that the voices of women will finally be heard.
As part of #Matexp I have made contact with some amazing people such a Flo, Gill, Rachel and Helen as well as fantastic midwives such as Jenny and mothers such as Leigh. All are doing amazing things to improve services for women often after personal experiences. Knowing that there are so many people who genuinely want to work to improve services and make care better and who truly value women has helped me heal and also restored my belief in maternity care. It has given me the opportunity to to tell my story and then feel part of improving things to make care given better for others something I am so passionate about. It has also given me confidence to be bold and change things in my own job and NHS trust as I feel supported by some amazing people. Seeing their successes has spurred me on and helped me believe that we can all make a difference.
More importantly #Matexp has given me hope. Hope that one day we will provide a maternity experience that is individualised, respectful, gives dignity and allows for informed choice. That puts a woman, her baby, her family and their needs first. It will mean birth experiences that do not result in trauma but that even under difficult circumstances will make a woman feel loved, protected and supported. Yes I have hope, because finally not only has my voice been heard but the voices of women everywhere will be heard, no matter who they are, what they do, or what choices they made. Why is this so important, because your birth experience stays with with you the good and the bad, it can have a profound effect on you as a family as you start on your journey as parents. All women, babies and families are special and deserving of the best maternity care possible. So join in, get involved and share your stories and your ideas. There’s exciting times a head in #Matexp and together we can make a difference.
by Helen Calvert / MatExp and Me / Comments Off on My #MatExp – two very different experiences!
As one of two breastfeeding champions for the NHS Change Day MatExp Campaign, I find myself talking a lot about maternity services. It is strange one for me, as although I speak to mums all the time about their maternity experiences, I actually have very little personal knowledge of giving birth on the NHS. With my first baby, I knew from the start that I wanted a homebirth. I had been following a homebirth email forum since before I got pregnant and had gained the impression that the NHS would make my life as difficult as possible if I decided to give birth that way (especially as a first time mum) so we opted to use an independent midwife. This was totally the right decision for me as I suffer from anxiety and have issues around loss of control so needed continuity of care and to be able to do things my way.
Second time around we couldn’t afford another IM, so we started out with the NHS. We wanted another homebirth and this time I was fairly confident that I could get the birth I wanted, being a lot more knowledgeable and also having already given birth at home. However, a few weeks in to my pregnancy a friend of mine told me about OnetoOne Midwives. Their service was exactly what I was looking for, and I was lucky that in 2013 I was able to self refer to them from Trafford. The lovely OnetoOne team looked after me from then on.
Sadly, when I was 38 weeks pregnant a routine check of baby’s heartbeat revealed an anomaly, and a week of scans and tests later gave us the diagnosis that our baby had Hypoplastic Left Heart Syndrome. Not only was homebirth off the cards but it wasn’t certain we would take our baby home at all. You can read all about our experiences with David here, but in terms of my #MatExp the staff at St Mary’s Hospital in Manchester were fantastic. I had a c-section, and as everyone was focusing on getting David out and into NICU, it was the most medicalised birth you can imagine, but I still felt respected and cared for, with things being explained to me every step of the way. Special mention goes to midwife Della and anaesthetist Andrew Heck who provided the kind of care that makes any maternity experience a positive one.
So going back to that first birth with my gorgeous big boy Edward, let me tell you my birth story as I wrote it back in 2011:
Birth Story – Edward Calvert enters the world
On Monday 31st January I was 42+1 and we were at the hospital for monitoring. We had agreed to be monitored to make sure that baby and I were still healthy, but knew that we didn’t want to book an induction just yet. We had a scan to check on the function of the placenta and then had 30 minutes of monitoring to check on baby’s heart rate, his movements and my pulse. Our lovely Independent Midwife Verena was with me the whole time, and confirmed that the monitoring showed no problems for either of us. We then had to wait to see a young obstetrician who outlined the hospital’s policy for women who had gone past 42 weeks. She confirmed that she would like to book me in to be induced, or failing that she would like me to come in for daily monitoring.
We confirmed that we understood the reasons for her requests but said that we would prefer to come back for monitoring on the Wednesday, and not to book an induction just yet. She respected our choices but due to her being fairly junior requested that we wait whilst she speak to a consultant. A lovely consultant then came to speak to us, and was more than happy to accept our choices once he had confirmed with us that we understood the situation.
That evening I made a concerted effort to relax and get myself into a good mental place to give birth. Having done a sweep that morning, Verena confirmed that everything was ready for me to go into labour – we just needed some contractions! So I lay down on the day bed in the nursery, put the lights down low, asked Phil to come and sit quietly with me and focused on putting myself into my relaxed state as taught by the hypnobirthing CD. Phil sat and read whilst I relaxed for half an hour.
At the end of that time, I asked Phil to get me a glass of water. No sooner had he left the room than I felt a pop and was pretty convinced that my waters had broken. I waited until he came back just in case I had lots of fluid, but when he helped me to stand up I only had enough fluid to soak a small patch into my jeans. I went to the loo and confirmed that the waters were not a bad colour, nor did they appear to contain any meconium. Phil phoned Verena and she said that most women go into labour within 24 hours of their waters breaking, so things should start to get going any time. This was 9:30pm.
At 10:00pm I felt what I was pretty sure was my first contraction, so I made a tentative note of it. I continued doing a jigsaw puzzle downstairs and just noted each contraction as it came, as at this early stage they weren’t painful. They were regular though, coming every 5 minutes from the start, and Phil phoned Verena to let her know what was happening. The contractions became painful fairly shortly, to the point where I had to concentrate through each one. Phil started filling the birth pool just before midnight, as he knew he could keep it warm so thought it best to make sure it was ready. He then phoned Verena at 12:30am to tell her that my contractions were getting stronger and were lasting around 40 seconds. She arrived at our house with Sara (second midwife) at 1:30am, by which time I was feeling a bit nauseous with the contractions and my back was aching. I was standing in the nursery, leaning on the day bed through the contractions, with my wave music on and watching a slide show of photos on the laptop that I had put together in advance to keep me cheerful!
Verena put the TENS machine on for me and that was beneficial although it felt strange to begin with. She checked me over, blood pressure etc. and also had a listen to baby’s heart. All fine, and my contractions were now a bit more spaced out (this often happens when the midwives arrive!) so Verena told me that I was definitely in early labour but that I wasn’t in ‘established’ labour as yet. She and Sara left at 3:00am and said they’d be back in the morning, but obviously we should call them if anything changed or if we needed support.
I spent the rest of the night kneeling on pillows, leaning against our bed and breathing through each contraction – they were now pretty painful and I was using the TENS machine through each one. I was only comfortable kneeling up, I couldn’t lie down at all, so I was dozing between contractions with my head on the bed. Phil got some sleep in the bed beside me, and I remember looking at him snoozing comfortably and being fairly resentful of how cosy he looked! I was sick a couple of times in the night, and Phil woke up to play pass the parcel with various bowls and receptacles! I woke him finally around 6:00am as I was fed up with dealing with the contractions by myself and I needed some support. We tried putting me in the shower to run warm water over my back, and Phil braced his arm against the tiles and I hung onto him during each contraction. Phil then phoned Verena at 7:30am to say that my contractions were every 3-4 minutes apart and were more intense – we definitely needed her to come back! Verena said that I could get into the pool if I felt it would help, and I got in as soon as I could! Was still only comfortable kneeling up so knelt in the pool, leaning over the side, and hanging on to the handles during contractions. I didn’t want to be touched at all whilst contracting, so poor Phil didn’t really feel like he could offer any comfort, but of course he was being fantastic and very encouraging.
Verena and Sara arrived back at 9:00am and put a warm, wet towel across my back to help with the backache. In my labour notes it says that I looked very relaxed but said that I didn’t feel it – I think I looked relaxed coz I was exhausted and was only awake coz I was contracting! Verena had a listen to baby’s heart – thankfully her equipment was waterproof so she could just pop the device into the pool and have a listen between contractions.
At 9:30am Verena told me that I was in or close to transition, i.e. the change between the first stage of labour and the second stage where you can start to get the baby out! I remember being delighted at hearing that, but am surprised reading the notes that it was 9:30am – I would have thought it was later in the morning that she told me that. You lose all sense of time in labour! Verena gave me a homeopathic remedy to help cope with the backache and exhaustion, and they all encouraged me to drink plenty of water. Unfortunately I couldn’t face much food, which was a shame as I desperately needed the energy.
Just before 11:00am I started to feel the urge to push, and got a bit more vocal during my contractions! Phil and Sara had been doing excellent work keeping the pool water warm and the midwives continued to monitor baby, but all this was background to me as my life was all about the contractions. I had a cup of sweet tea as everyone kept encouraging me to get in anything that could give me some energy. Verena has put down in my labour notes that Cleo the cat turned up outside the nursery door at this point to have a concerned yowl, but she wasn’t allowed in the room. I do remember hearing her make her presence felt! It was around this point that I began to push a little during contractions – not a choice, just something my body felt it was time to do. By 11:30am I was getting a strong urge to push with every contraction.
Ten minutes later, Phil lit some candles and Verena noted they were all getting ready to meet baby. I am of course taking all of these timings from my labour notes – I had very little idea of what was going on and certainly no clue of time! It was all about getting through the contractions and resting as much as possible in between. Verena thought a change of position might help with the pushing, so I stood up in the pool supported by Phil. All the signs were good that baby was ready to come, and everyone was encouraging me to push and telling me how well I was doing. I went back to kneeling in the pool and Verena has put in my notes that I was pushing very effectively. I remember it was bloody hard work!
At 12:30pm Verena gave me another homeopathic remedy to help with the pushing and I continued to use all of my efforts. At 12:50pm Verena has made a note to say that when she was listening to baby’s heart “baby trying to kickbox my hand away as if to say go away, I am coming out!!”. I changed position again so that I was lying on my side in the pool, still with my head on the side – change of position suggested by the midwives as all the efforts at pushing were not getting baby “round the u-bend” as they put it! I then tried squatting in the pool, but complained that the contractions were not long enough to give me enough time to push effectively – I was getting in perhaps three good pushes and then the contraction subsided when I felt I could do with just one more push to make it effective! Verena gave me a homeopathic remedy to assist with this (all of these remedies were with my consent of course).
It was becoming clear that a change was needed as we weren’t progressing despite my best efforts at pushing. I therefore got out of the pool just after 1:30pm – this was incredibly hard as moving during a contraction was impossible so it was finding the time between them to get me out and moving! Phil and Verena half carried me into the bathroom and sat me on the loo, as this is a natural place to push and this is often an option used in homebirth. I told them “he is coming” and I think I must have felt him crowning (i.e. the head pushing its way out) at this point. Unfortunately, although the head started to emerge it then retreated back again (not unusual) which was of course discouraging each time it happened as each time I knew I had to get it back again! The midwives moved me onto all fours on the floor of the bathroom and got some towels ready to catch the baby.
At 1:50pm baby’s head was born – I remember Verena saying “we have eyes, we have a nose, we have a mouth” and I just felt so relieved as I knew his head was finally out and couldn’t go back in again! Verena has noted down that baby was “blowing bubbles” and he looked just like Phil! What I remember very clearly is thinking, okay I have a moment’s respite now before I need to push out his shoulders, and at that point baby decided to have a look around the bathroom. The sensation of him moving his head is indescribable – I think I asked him to stop, or maybe I just thought it, but I didn’t appreciate his enthusiasm at that point!
Three minutes after his head was born the rest of baby emerged – he had his hand up by his face which could explain why pushing him out had been such hard work. He lay on the floor looking up at me, I was on all fours looking down at him and both of us were a little stunned! He needed a bit of a rub with the towels to get him going, and then he cried and was clearly fine and healthy. Verena asked if I wanted to hold him, and I realized that yes I did – it hadn’t occurred to me, I was too stunned!
Baby and I had some skin-to-skin time and the midwives helped me to sit up on the toilet, as I had been kneeling up almost continuously since the night before and my legs were shaking and exhausted. Unfortunately, as I moved to sit up there was a gush of blood – nothing to cause concern, but it did make a pretty effective mess of the bathroom. Thank goodness we were in a room that was easy to clean! Verena took some photos of me and baby, and of Phil with the two of us – these pics will never see the light of day as I look unbelievably awful – but I also look pretty happy!
The cord stopped pulsating but I felt a bit dizzy so they helped me to lie down on some towels and pillows on the landing, still with baby cuddled up with me, and they then tied the cord with our homemade cord ties. Phil cut the cord and said “I declare this baby open” – he was in very high spirits! Sara had made tea and brought up some biscuits so we all had a snack – she hadn’t been able to get in the bathroom as Phil and Verena were in there with me so she missed the actual birth, but could hear it all happening from outside the door! Whilst I had a nibble of something to eat Phil had his first cuddle with baby… and we agreed to call him Edward.
Phil had taken off his T-shirt so he could have skin-to-skin with Edward, and Verena was attending to me as I still needed to birth the placenta. I was contracting slightly and Verena was asking me if I could push out the placenta, but bizarrely I had completely lost the notion of how to push! I just couldn’t work out how to do it! Verena moved me into a couple of different positions again, but by 2:45pm the placenta still hadn’t arrived, so I agreed to the syntometrine injection to encourage the process. Verena gave me the injection and then the placenta arrived about a minute later, so it would have come of its own accord anyway but there you go. I didn’t suffer any nausea with the syntometrine so no harm done.
Verena then helped me to have a quick shower, followed by me being helped into bed – bliss! Verena examined me and said that I had a small tear but that I didn’t need any stitches. By 3:30pm Verena had helped me to latch on Edward for his first feed, whilst lying together in the bed. Very special moment. Phil was making sure everyone had refreshments and they were all encouraging me to have orange juice and things rich in iron due to my blood loss. Verena asked if I wanted to eat a little of the placenta, which I know sounds gross, but I had considered it prior to labour. I agreed as it is a very iron-rich product, and Verena gave me three or four tiny pieces that I washed down with water.
Edward was weighed and checked over – he came in at 8lbs 13oz. Verena and Sara made sure we were all happy and healthy, gave us some advice for the first night, reassured us they would be back tomorrow then they left the house just before 5:00pm. The Calvert family were left together and couldn’t have been happier.
Our constantly evolving MatExp story has since been published in NHS #100daysofchange . If you are in any doubt about the difference NHS Change Day makes, take a look at these wonderful stories.
So I am delighted to introduce my J*DI ‘partner in crime’ Florence Wilcock, a.k.a . #FabObs Flo @fwmaternitykhft, who tells her powerful and very human story:
3am the phone rings “There’s a massive obstetric haemorrhage in maternity theatre 2”, I leap out of bed, throw clothes on and get into the car. My mind is racing through causes of haemorrhage, how severe is it? what have the team already done? As I drive into work, I ring to speak to the midwife in charge seeking information and checking off a mental list: pulse, blood pressure, estimated blood loss, blood cross matched, consultant anaesthetist. Brain whirring. By the time I get there, it could be sorted or life threatening, which will it be tonight? Drive carefully, ignore your heart pounding, the adrenaline flowing; don’t be distracted, people are depending on you.
In my role I might be invisible to you if everything is going well and all is normal. You will never meet me, know my face or name, despite my being an essential part of the team and often the lead. One component of my job is to do nothing, to stand back, to not intervene and to teach others how to do likewise. My job is to master the art of being there only at the critical time, to run in and save the day, keep calm whilst doing so and to never get that judgement wrong. An impossible balance of risk vs. choice, art vs. science, clinical outcome vs maternal experience.
My name is Florence. I am an obstetrician.
I’d like to tell you the story of two births.
Birth 1: Twelve days overdue with a first baby, this mother expected a straightforward normal birth. That was what her mother and grandmother had experienced. Her waters broke before labour. The mother was told she had to be induced. She reluctantly went into hospital where she started a hormone drip. She later had an epidural as the midwife kept pressing her to. She had an emergency caesarean after twelve hrs of drip, being only 3cm dilated; it felt the inevitable outcome. The epidural didn’t work, so she had a spinal for the surgery. On the table she felt disconnected, almost like an out of body experience, she felt vulnerable. When the baby was born, she was disinterested and didn’t want to hold her. She was in pain after the surgery but the staff didn’t believe her and told her she had already had the maximum dose of pain killers. She lay rigid and still in pain, watching the clock move slowly until she thought she could reasonably ask again. At home it took months before she could talk about the birth without crying. She had failed.
Birth 2: Same woman, four days overdue planning a VBAC (Vaginal birth after caesarean) contractions started, went to hospital overnight. Next morning, 3cm dilated, offered the birthing pool. Wonderful warm water, giggling with gas and air and the midwives keeping the obstetric team out of the room so they wouldn’t interfere. Sadly after many hours 5cm, so got out of the pool and had an epidural and her husband kept her entertained reading from the newspaper. Later, still 5cm dilated, choices offered, caesarean or hormone drip, joint decision: caesarean now probably safest. A wonderful anaesthetist distracted her with football chat and suddenly a baby daughter was here. Exact same outcome: emergency caesarean, healthy baby girl; exact same hospital: but she felt she’d had her opportunity for a VBAC. She had been listened to, supported, valued, and positively involved in her care.
That mother was me. My name is Florence. I am a mother.
At any social gathering, I inevitably get a blow by blow account of at least one birth story, if not several. A birth experience stays with us forever, we remember it like it was yesterday, it is a pivotal moment in time. I am privileged to witness incredibly special moments and emotional events on a daily basis. Often when I listen to these birth stories, we obstetricians and midwives seem to be portrayed as the villains of the piece, especially the obstetricians. I find this negative stereotype particularly annoying. No doubt there are less empathetic or more obstructive obstetricians as there are imperfect members of any profession, but most will be hard working and diligent and simply trying to do their best for women in their care. From my own personal experience both as an obstetrician and a mother I can see the importance of maternity experience. I often wonder: how have we come to this polarised position? how did maternity staff become the bad guys, upsetting the very women we are trying to care for and what can we do to change this?
How the #MatExp campaign was born
Gill Phillips and Florence Wilcock
For this reason I volunteered to lead the London maternity strategic clinical network sub group on ‘patient experience’. London had six of the seven worst performing Trusts in the country in the 2013 CQC Maternity women’s survey; we needed urgent action. In contrast, at Kingston Hospital NHS Foundation Trust where I work, we have had consistently excellent feedback from women in our CQC survey. I thought this was perhaps an opportunity to work out what it was we were doing well; to ‘bottle it’ so that others could copy.
I wanted to find an innovative way to explore the issue and ignite the feeling that experience is everybody’s business including women themselves. I had recently started tweeting (My NHSChangeday 2014 pledge) and stumbled across Gill Phillips @Whoseshoes and the idea for #MatExp workshops was born.
With the support of Kath Evans and a team at NHS England London, Gill and I have collaborated to design a bespoke maternity version of her ‘Whose Shoes?’ board game. We have used real scenarios from users and staff to examine maternity experience from all angles and perspectives.
The aim is to use the workshop as an ‘ignition tool’ to build connections and relationships across the broad maternity community. We want to enable true collaboration, co-design and ongoing conversations to improve maternity user experience.
Poem by Gill Phillips written directly from a ‘brainstorm’ email Flo sent when we were compiling scenarios, after a middle of the night emergency
We have run 4 of 5 pilots in London, bringing together people from the whole broad maternity community: users and their families, acute and community staff, managers, commissioners and lay organisations. Getting everyone in mixed groups round a board game in a relaxed environment, babies welcome, refreshments on hand, gets the creative sparks flying. It is essential to remember that each person is present in multiple capacities; professionals are also mothers, fathers, sisters, friends and family with their own stories and birth experiences; users often bring knowledge and expertise from other aspects of their lives such as job, culture, education that are invaluable too. Respect and equality are essential ingredients; discussion starts from the assumptions that ‘best can always be better’ and ‘Wrong is wrong even if everyone is doing it, right is right even if no one is doing it’. We have been fortunate to have wonderful graphic facilitation by Anna Geyer @New_Possibiliti which both provides excellent feedback on the day but also a permanent visual record of actions which goes on generating new conversations.
At the end of each workshop each attendee is asked to pledge what they as an individual will do differently to improve maternity experience. This brings a personal sense of responsibility for the actions, the outcome is not the sole responsibility of the traditional hierarchical leaders but of us all.
“The resulting actions are already taking us in directions I could never have imagined such as user co-design of maternity notes, improving antenatal information for fathers and starting a midwifery team twitter account.”
Despite believing myself to be already very ‘person centred’, as I work on the project I am finding a succession of small changes spilling into my own everyday practice. I am thinking increasingly carefully about the choice of language I use and the way we behave. No more ‘are you happy with that?’ when explaining a plan but ‘how does that sound to you?’; explaining to women why we have come on a ward round; having a father in theatre when his wife had to have a general anaesthetic so that they didn’t both miss the birth; using the intense listening I have learnt in coaching to understand women’s perspectives in my clinic.
Through social media the #MatExp project has generated interest from women and maternity staff up and down the country. We have held a train-the-facilitator day to look at how to roll out the workshops both in London and more widely. But the conversation has already become much broader than the board game, with people from the maternity community energised to talk about maternity experience and actions they can take. The project appears to be prompting people to speak up, share and act on their ideas. Linking with NHS Change day on 11th March is a fantastic opportunity to spread the message and get those vital conversations started.
The beauty of #MatExp is anyone can do anything, however big or small, whoever you are: user, partner, community group or NHS staff. Your action could be one of those simple suggestions listed or could be your own idea. The sky is the limit! Imagine if we designed maternity care from scratch what would it look like? Would it even be called maternity? How about transition to parenthood? Every action we each take, however small, keeps the #MatExp conversation going and makes a small improvement. If we all take action together, we have huge potential to improve maternity services and an experience that has an impact on us all.
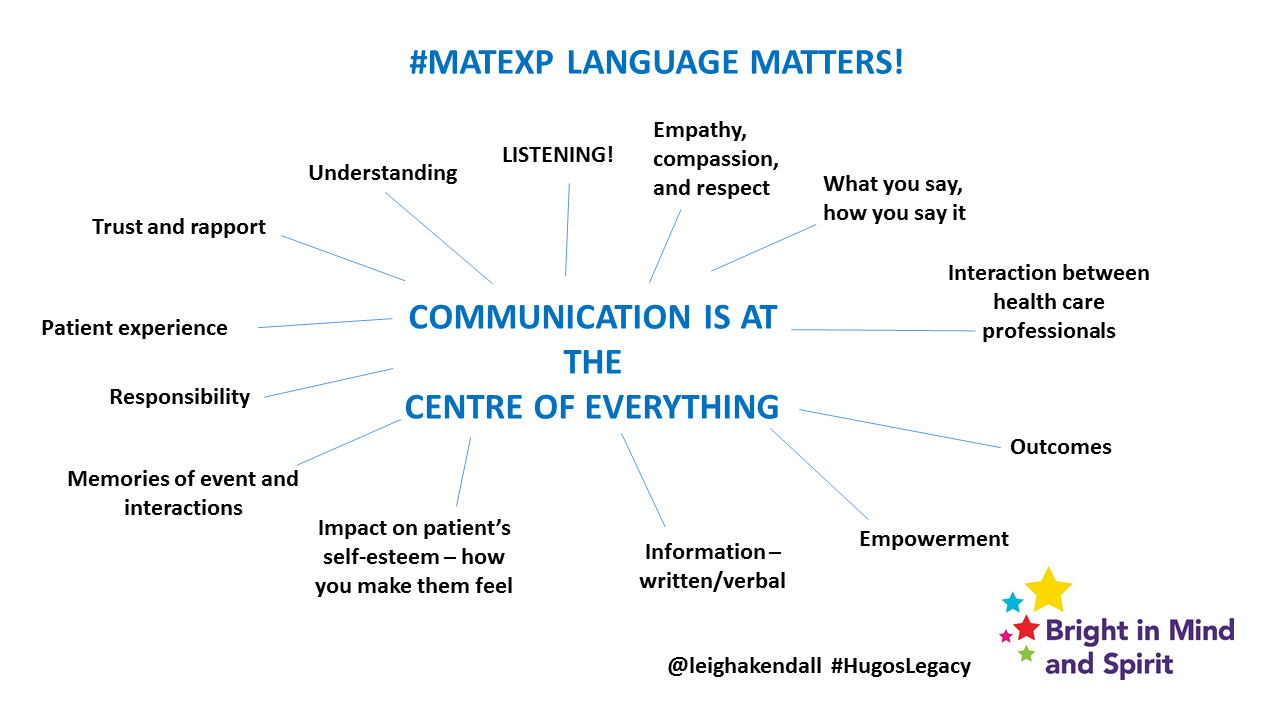
Being in any healthcare environment for any reason can feel disempowering for a patient. Effective communication between healthcare professionals and patients can help build trusting relationships, improve patient outcomes and patients’ experiences.
Communication is at the centre of everything, and no more so than in a healthcare environment:
Continue to raise awareness of the importance and impact of effective communication – verbal and written – through all appropriate channels (including my blog, on social media, engagement workshops, for instance). While healthcare communication is important in any specialty, as a result of my personal experiences my focus is on maternity and neonatal unit environments.
Empower women to feed back about their experiences – positive and negative – to help health care professionals improve patient experience (part of this action includes discussing how to make the process of giving feedback easier, and meaningful).
I have been proud to be involved with the #MatExp campaign for the past few months. #MatExp is a campaign led by healthcare professionals and users alike, aimed at identifying and sharing best practice across the country’s maternity services. If you check out the hashtag on Twitter, you will see it has already been generating lively discussion about what needs to improve.
My passion for appropriate language and effective communication stems from my years of experience as a communications professional in the NHS. This passion was enhanced as a result of my personal experiences as a patient and as a parent in 2014.
For the benefit of those unfamiliar with my story, in February 2014 I was diagnosed with the rare, life-threatening pregnancy conditions HELLP syndrome and pre-eclampsia when I was just 24 weeks along. The only cure is for the baby to be born, and my son Hugo was born 16 weeks early. My beautiful son was too small, and premature and sadly died at the age of 35 days.
While nothing differently could have been done from a clinical perspective, there were several incidences where our experience could have been less stressful, and additional upset avoided if there had been better communication. That is why I set up Bright in Mind and Spirit (it is what Hugo’s name means), to raise awareness of these issues.
This slide explains more about why language matters, and why healthcare professionals should care about getting it right:
Feedback from many other women on social media and through their own blogs reveals I am not alone in wishing for better communication in my maternity experience. These women had every kind of pregnancy and birth experience you can think of. The one thing we share in common is the impact poor communication and choice of vocabulary by healthcare professionals had on our maternity experience.
Language can have an enduring impact, with things that were said to women when they were giving birth to their babies staying with them many years later.
This slide describes the language we want to ban, and the kind of language we would like to see more of:
Medical jargon can be confusing and bewildering. In addition, some terms may impact a woman’s self-esteem.
Terms like ‘failure to progress’ and ‘incompetent cervix’ might be perfectly proper medical terms, not intended to be personal. But think about it for a moment: these terms describe a woman’s physiology. Women therefore cannot help but take personally such terms. In the context of pregnancy, where expectant mothers want to do everything possible to protect their babies, such words can inadvertently convey a sense of blame, leading the woman to feel she a failure or incompetent, rather than elements of her physiology that are beyond her control.
The words and terms in this column can make a woman feel like she is not in control of her body, her care, or decisions that are made. A bit of a walking womb. Doesn’t sound very nice, does it?
The examples given in the ‘language we want to see more of’ column outlines some simple ways to help a woman feel more in control of her body, an equal partner in her care, and involved in decisions. Sounds much better, doesn’t it?
Healthcare professionals of all disciplines need to reflect that each patient is an individual, with their own experiences, values, hopes and fears.
There is so much discussion around language in maternity services. For instance, women have raised points about choice (some women have little choice about how or where they give birth, for a variety of reasons); risk (which sounds scary – often it means only ‘possibility’); and ‘normal’ birth (the notion that there is a ‘right’ way or place to give birth). The vocabulary we use to describe birth is crucial for helping women feel equal and empowered. It could also help remove the polarisation of views between ‘normal’ birth always being best, interventions always being harmful, and take some of the fear out of the delivery room.
Empowering women to feed back about their experiences is the second part of my action. Healthcare professionals may not always be able to recognise that experience needs to be improved, unless they receive feedback. The problem is, the traditional feedback processes can often be onerous, stressful and result in unsatisfactory results for the complainant.
The NHS complaints process is complex, for many reasons, and can include cases of straightforward feedback to serious incident investigations and everything in between. The whys and wherefores of the complexity of the process is not a topic for this post. However, there are some simple considerations individual providers can implement to help the complainant feel like they have been listened to, been taken seriously and that they matter.
My personal experience of the complaints process from a hospital, a GP practice, and a mental health provider is the opposite. More stress and upset was caused by written responses that were impersonal, formulaic, and failed to acknowledge the impact the experiences had on me. The tone of the letters felt like board reports, and that the response had to be written so it could be added to a chart.
People composing these responses need to take a step back and appreciate that while there are statutory points to be made, facts to be stated, the recipient is a human being with feelings that do not fit into a chart. Think about the language of the letter and how things are phrased to help the complainant feel like they have been listened to, been taken seriously, and that they matter. Where appropriate, also advise the complainant of actions that are being taken as a result so they can be assured taking the effort to give feedback was worth it.
It is difficult to write this post without some reference to the Kirkup Report. There is so much I could write about it, but this post from Birthrights provides a useful insight into the impact that communication had on the care of women and babies at Morecambe Bay – with tragic results.
Improving language and communication will take time, and a shift in culture. In many cases there are no easy answers. However, recent social media discussions (with midwives, obstetricians, professionals from other specialties, as well as other users) about language have been heartening. It is heartening because the discussions between healthcare professionals and users have happened, and on such a public forum. It is heartening to see language being thought of, and the link between communication, outcomes, and patient experience being recognised.
The main point to remember about communication in healthcare is to consider how you would like to be treated yourself. You’re likely to want to be treated with compassion, empathy and respect, aren’t you?
by Leigh Kendall / MatExp and Me / Comments Off on MatExp and Hugo’s Legacy
A significant part of Hugo’s legacy includes improving experiences of maternity services for women who have a traumatic birth, and/or whose baby is cared for in a neonatal unit. My particular focus is on making sure language, communication and information is clear and effective at this time, which can be bewildering and upsetting for mums (and dads).
Twitter is a fantastic networking resource, and for the past few months I have been tweeting with a group of health care professionals (HCPs), NHS change agent folk, and other women who, like me, are passionate about helping improve other women’s experience of maternity services.
I was delighted to meet Flo, Gill, Kath, and Carolyn after tweeting for so long. Being able to talk in sentences longer than 140 characters was refreshing! My good friend Michaela was also at the event, and it was lovely to catch up with her.
There are a series of #MatExp events, which seek to get service users and HCPs together to discuss experiences. I went to an event at Queen’s Hospital in Romford, which is part of Barking, Havering and Redbridge University Hospitals NHS Trust.
It is an impressive hospital: the reception airy is airy and colourful. Someone was even playing a grand piano.
The attendees for the event included trust staff from a range of professions and grades, as well as service users. We were sat on round tables: when I introduced myself, I was amazed that someone on my table said they followed me on Twitter. Hugo’s story is getting around!
A comment in the opening speeches about “pregnancy not being an illness” raised my hackles. Yes, for the vast majority of women pregnancy and birth is a natural, wonderful life event. But for some women, pregnancy and birth can be a source of great trauma. Indeed, pregnancy can make a minority of women very ill indeed, as I can attest.
The speech was full of aspiration and positivity, which is understandable in the context of the hospital seeking to become one of the country’s highest-performing maternity services (a few years ago they ranked amongst the worst). However, speakers do need to be mindful of the range of women who are likely to be in the audience. Pregnancy and birth does not always go to plan – there are times when it is unavoidable, it is no one’s fault, and women like me do appreciate this being acknowledged. That’s my soap box moment – it is a point of sensitivity.
Each table played the Whose Shoes game. The game is simple – you roll the dice, move your shoe around the board, and discuss the scenario related to the colour shoe you land on. The scenarios involve getting in the shoes of a mum, or a range of HCPs.
My table’s scenarios generated some interesting discussion. For example, we talked about perception around labouring women being ‘not allowed’ to do certain things. The HCPs said they never knowingly say women are ‘not allowed’ to do anything, which is interesting in terms of perception.
In any healthcare setting, a patient may feel disempowered, and feel like they have to do what they are told. Think of transactional analysis: even if the HCP and patient might have an adult/adult relationship in a social setting, a healthcare environment can transform that relationship to a parent/child relationship.
Think about how parents tend to talk to children. The children are given parameters, boundaries, and if they disobey they may find themselves at the receiving end of a wagging finger or sharp tongue. That’s not fun as a child, and even less so as an adult. It’s a key example for HCPs to consider language – what they say, and how they say it.
Of course, as the table discussed, there are some situations where women are told they shouldn’t do things, and for good reason – for example, directly before or after a Caesarean section. In any such situation, the table agreed, it is vital for the HCP to explain the reasons, as well as any suitable alternative options and what they might mean. The HCP can use active listening (paraphrasing what the woman has said) to check their understanding. That doesn’t take long, costs nothing, and has the benefit of helping the woman (or any patient) feel like an equal partner in decisions about their care.
Equality was the subject of another scenario. The scenario related to the needs of minority ethnic women, but sparked a wider discussion about equity of care. The consensus was that women should not be treated equally. That might sound counter-intuitive, but think about it for a moment: every human being is an individual, with their own individual hopes, dreams, fears and needs. In a maternity setting, you and the woman in the bay next to you might be there for the same reason, but because you are each unique individuals your needs are unlikely to be the same.
For example, I was treated differently in some ways to the other mums when I was in the post-natal ward after giving birth to Hugo. I was grateful for the private side room, meaning I avoided being in a bay with mums who had their babies with them. However, the staff didn’t consider all my needs as a new mum whose baby was being cared for in the neonatal unit: I was left waiting for too long to see the doctor on their rounds, for instance, which meant I missed precious time with my seriously-ill baby.
The event concluded with the key points from each table’s discussions included on a giant piece of paper by a graphic facilitator. You can see some of the points in the photo below. Appropriate care for women like me who have had a traumatic birth and/or whose baby is in a neonatal unit is a focus for me and I would have liked to have seen more on that. However, if there is an overall focus on doing everything possible to meet individual women’s needs, as well as other points of feedback, then this will hopefully improve as part of that.
There was then a challenge to decide what the hospital’s maternity services wanted to be known for. I was relieved the suggestion of ‘a positive birth experience for every woman’ wasn’t accepted, because they would be setting themselves up to fail and more importantly, setting women who don’t have a positive experience (for whatever reason) to feel like they have failed. “Having pride in our delivery of care with excellence” was the chosen slogan. While positive, I am on the fence about it (it is pretty standard) but to be fair it was chosen quickly by mass of people who were at the end of a long day.