Huge thanks to the fab(!) ‘FAB NHS Stuff’ team for setting up a dedicated ‘Whose Shoes’ collection to collate and share some of the FAB stuff that we do, including many #MatExp examples.
The collection is growing! Have a browse – you are bound to find lots of easily transferable ideas that will work for you, not least in our various booklets of case studies.
Originally posted September 26, 2016 by Leigh Kendall
This post was written by Leigh Kendall, mum to Hugo who sadly died aged 35 days. The post was originally published on 26 September, 2016 on Leigh’s now defunct personal blog. You can get in touch with Leigh on Twitter at @LeighAKendall.
Nobody’s Patient workshop: St George’s Hospital – 26 Sep 2016
Friday September 23 was a special day, one I have been waiting on for a long time: the Nobody’s Patient workshop at St George’s Hospital.
The workshop is a key part of the Nobody’s Patient project and received funding from the Maternity Review Challenge Fund . The project evolved from the grassroots social media change platform #MatExp, and was inspired in part by my experiences with Hugo.
My beautiful Hugo
Bringing Nobody’s Patient to St George’s, where Hugo was born, lived and died is an achievement that means so much to me that it is hard to fully express using mere words.
The aim of the workshop was to get health care professionals involved in caring for families like mine to understand more about our experiences, and to make pledges to improve experiences for other families. I can’t change what happened to us, but through #HugosLegacy I wanted to help future families’ difficult experiences be a tiny bit easier.
The first workshop, in Kingston in early July 2016 was a huge success – everything was crossed for St George’s to emulate that. I was delighted to see so many people attending the workshop – all busy people prioritising the workshop over the million other things they have to do.
The workshop got underway: the room was full of buzz and ideas. Participants barely even stopped for refreshments so engrossed were they in the scenarios and discussion. All the scenarios are sourced from real people’s real experiences, which makes them very resonant, relevant, and often emotional – for both negative and positive reasons.
Communication was of course a topic that underpinned many of the discussions. Some of the key points from the table I was on include:
The suggestion that doctors could use drawings to help parents understand their baby’s condition. Parents are tired, stressed, and emotional – being in the NNU can feel like you need to gain a medical degree within days, and there is so much terminology to learn. Parents are constantly anxious, and their precious baby being attached to an array of beeping machines that are keeping their baby alive adds another level of terror. Visual aids such as drawings of anatomy can help parents understand – and in turn these drawings can help parents explain their baby’s condition and prognosis to family and friends, too. Doctors shouldn’t worry about their art skills – it’s about the concept rather than it being perfect! Anything that helps parents grasp complicated concepts is positive. There are some worries about notes and the formal medical record and governance, but the consensus was that drawings used as part of a conversation with parents are separate to the formal medical notes.
NNU mums often have difficulties receiving the necessary postnatal checks (whether or not they were ill during pregnancy, as I was). NNU mums’ priority is their baby, but their health matters too: they need to be as healthy as possible so they can be there for their baby, whatever the outcome. Our table discussed the concept of a ‘virtual ward’ where NNU mums could have their postnatal checks by identified professionals who crucially would have some training in the needs of NNU mums. Emotional and psychological needs of NNU parents are very often missed.
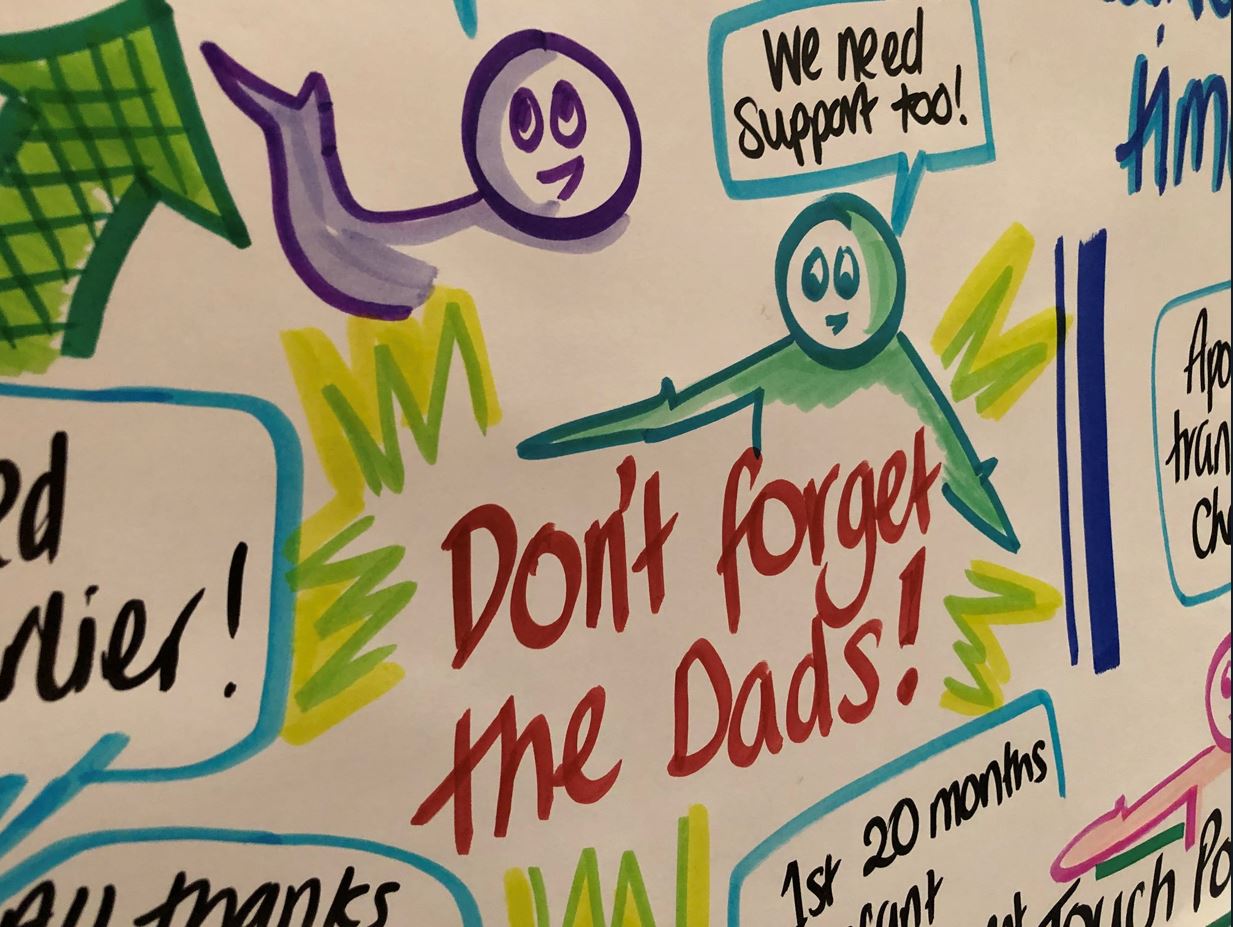
Dads and partners matter! Our table discussed how dads can be left out of the equation. There are times where they have been left alone after a traumatic birth, with blood everywhere and the in the delivery room looking like a scene from a horror film, their wife/partner and baby having been whisked away. The group talked about how in an emergency situation the room will be full of a range of professionals doing what needs to be done. Even if the procedure or equipment is routine, it may seem terrifying to the relative. Often after the emergency all the staff will leave the room with the patient, or go off to attend to other matters. Someone needs to remember to speak to the relative, debrief them, keep them updated, and give them information – not leave them standing panic-stricken.
I was heartened, especially after the disjointed nature of my own care, to see the dedication of professionals from various specialties keen to work together to give these mums and families the best possible experience and minimise additional stress.
Gill made this fab video of the awesome graphic facilitator Anna rounding up the feedback
In case you don’t have time to watch the whole video, some highlights amongst the many excellent pieces of feedback and pledges are:
A method of parents keeping an eye on their baby even when not physically present, eg FaceTime. This would have been so helpful to me when I was in intensive care in the hours before I was able to go and see Hugo, and for both Martin and I when we had to go and rest. Every neonatal parent needs to rest, and some parents need to go to work and/or care for other children too, so making use of technology would help parents feel able to be close to their baby at all times.
To see the mother and baby as one unit. The postnatal ward and NNU currently do not communicate well with each other; these links need to improve. In particular, the postnatal ward needs to better recognise the needs of NNU mums with things like expressing breast milk; food, emotional support, and being in the NNU with her baby as much as is possible.
Ideas to help parents understand and get involved with their baby’s care as much as possible, for example emoticons on the incubator to signify how the baby is doing.
The need for kindness, empathy, and understanding for any parent who is seriously ill during pregnancy, whose baby is cared for in an NNU, or whose baby dies at any stage during pregnancy.
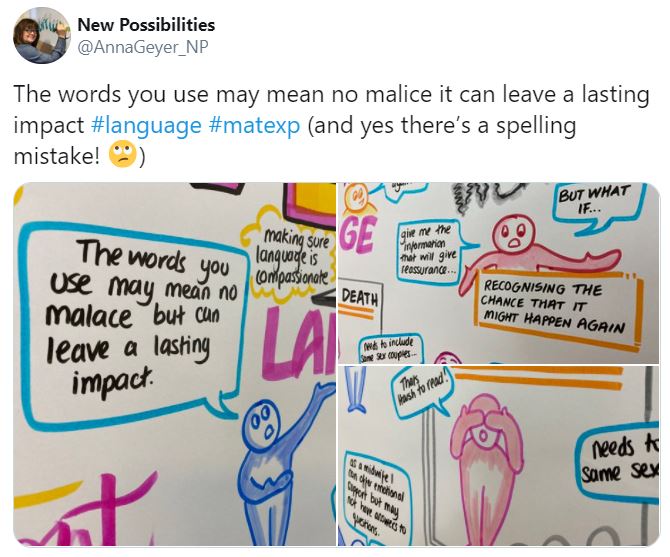
Graphic by Anna Geyer, New Possibilities
After the conclusion of the workshop, we spent a lovely couple of hours in the First Touch garden, soaking up the glorious sunshine. This garden was designed by a NNU dad (whose lovely wife is also the charity’s director) and won a prize at Chelsea. The garden was moved to the front of the hospital for everyone to enjoy.
Flo, me, Catherine, and Gill in the First Touch garden
I would like to say a heartfelt THANK YOU to everyone who made this workshop a reality through organising it, and to everyone who attended. Martin and I cannot change what happened with me, and we cannot bring Hugo back. Helping other families through Hugo’s legacy helps us by knowing that Hugo can never be forgotten, and that his life has had purpose.
St George’s has been brilliant at listening to the feedback I have given them about the experiences of my own care and Hugo’s care, and has already implemented many improvements where necessary. I shall always be grateful to the hospital for saving my life, and for giving us 35 precious days with Hugo. The hospital and the staff who work there will always have a special place in my heart.
And, of course, Nobody’s Patient is about more than me, Martin, and Hugo. It is about ALL families who find themselves in a similar situation. We are working together to help prevent other families falling between the cracks of services, and avoid unnecessary additional stress and upset.
The St George’s and Kingston workshops are part of a pilot that we hope other hospitals nationally will take on board.
Because nobody should feel like they are nobody’s patient.
Leigh Kendall talks about the Nobody’s Patient project, Hugo’s Legacy, and #MatExp
We recently ran a virtual Whose Shoes? event around baby loss, in conjunction with Gloucestershire maternity team and Sands bereavement charity. It was originally planned as the second of a 2-part event to use Whose Shoes to test out the ‘National Bereavement Care Pathway’ (NBCP) and identify any gaps.
‘Event 1’ went ahead on 6 March 2020, in Colchester …
The Colchester event was extremely powerful, with a lot of buzz in the room, hugs, good support and some powerful outcomes. That sadly feels like a different world now, doesn’t it?
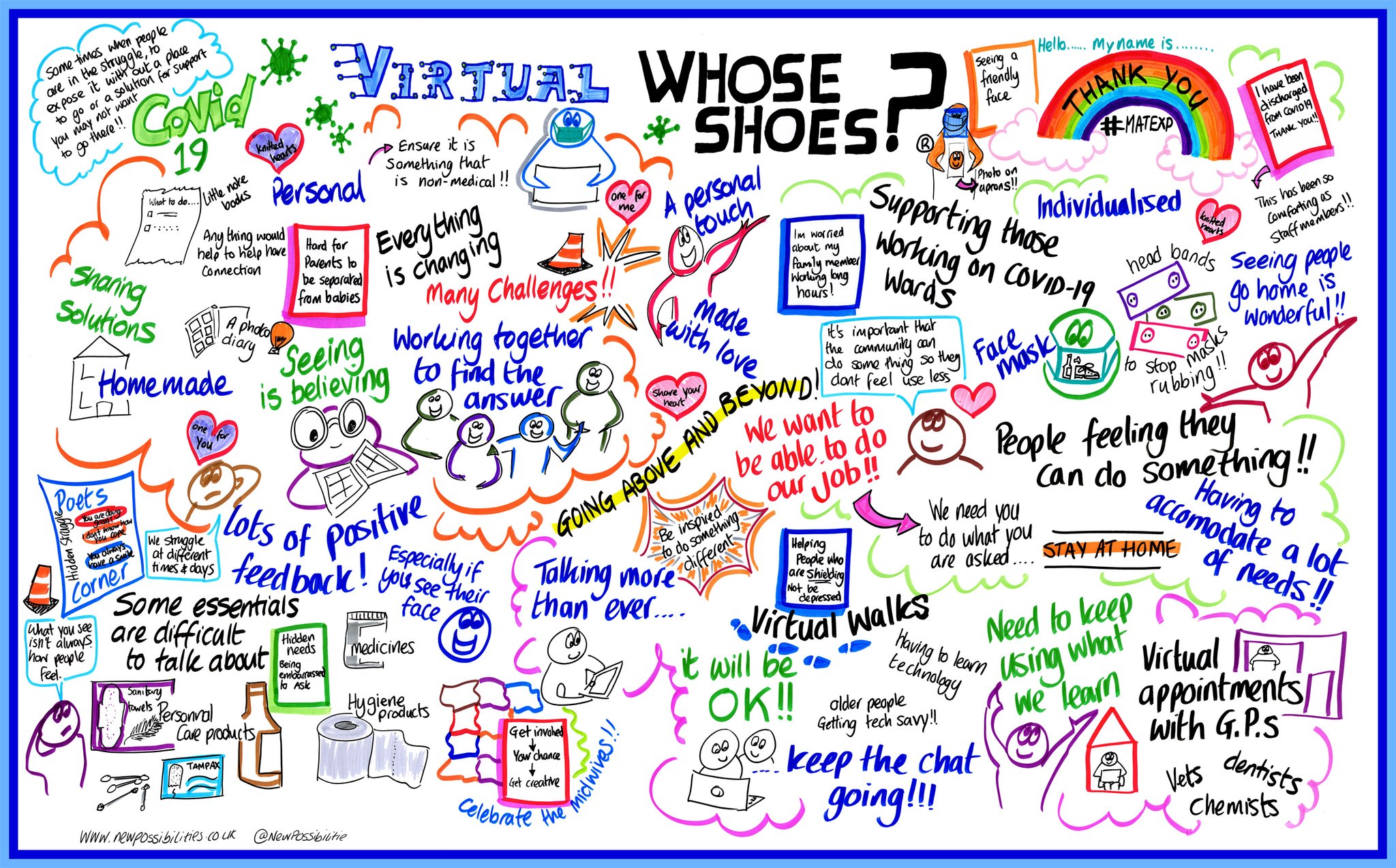
Anna Geyer, Director of New Possibilities, made this film of the event:
‘Event 2’ in Gloucestershire was meant to follow a couple of weeks later, but we all know what happened in the meantime. Covid struck and it took us 10 months to work our way through how to run an event of this importance and this sensitivity online.
I will fast forward and bypass how we developed #VirtualWhoseShoes, and all the twists and turns along the way …
Suffice to say that it was thanks to the dedication and perseverance of everybody that we managed to make the event happen. Dawn Morrall, Assistant Director of Midwifery & Nursing and the Clinical Improvement Lead of the South West Clinical Network, checked out the emerging virtual experience, and insisted that it should remain as a Whose Shoes event.
Dawn is one of the people who really ‘gets’ Whose Shoes. Dawn also has a great track record of following up on the quality improvement actions in order to get the most from the events … so we love working with the team in Gloucestershire!
I am hoping Dawn will write a case study about the outcomes from our previous events – and from this one in due course!
Online sessions take a huge amount of preparation. We had a lot of supporters, both in the room and following us on Twitter. #FabObs Flo Wilcock, consultant obstetrician, and Marc Harder had been the people who originally initiated the events:
Despite detailed preparation over many months, we didn’t really know how many people to expect, or the mix of people. Healthcare professionals are obviously so busy at the moment, with the pressures on the NHS due to COVID; people are feeling isolated during lockdown and missing the normal support available from family and friends. They are also ‘Zoomed out’, as the pandemic drags on.
It is hard for any new parents / parents-to-be at the moment, let alone people experiencing bereavement, so it was wonderful that Kerri and many others were keen to join. THANK YOU!
I was amazed. We had about 60 people on the call. It was wonderful and very moving to see so many bereaved parents joining us, alongside healthcare professionals, chaplains, people from SANDS, volunteers, medical photographers, a GP, a funeral director, and many more…
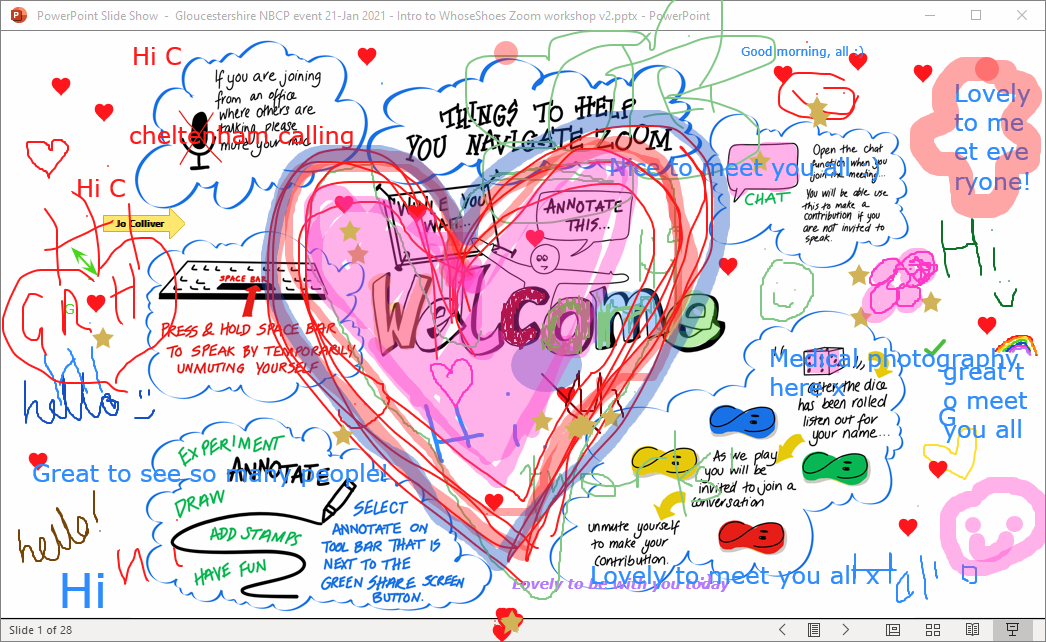
We started off with a gentle activity – colouring! It helps people learn Zoom skills that we then use later in the session to annotate certain screens. But it also feels relaxed, encourages people to turn on their mics and speak, adds a bit of colour and creativity and helps set the right tone for the session.
Coproduction in action – colouring the Welcome screen!
Clare Worgan from Sands (stepping in for Marc Harder, who has championed this work – get well soon, Marc!) gave a wonderful introduction about the National Bereavement Care Pathway, sharing many links and resources, including NBCP e-learning modules. A bereaved mum herself, Clare is passionate about bereavement care. Her authenticity and keenness to help others shone through.
And then a very moving introduction from Deborah Lee, the Chief Executive. Again Deb spoke from the heart, welcoming everyone to the session but also embodying our #NoHierarchyJustPeople mantra by sharing her lived experience story of baby loss.
It was wonderful that she was able to prioritise sharing this vulnerability and helping others, alongside juggling vital meetings to run the hospital! We all really appreciated it and it set the context for the event perfectly. Deb has generously given us permission to share her talk, as appropriate, at any future sessions too.
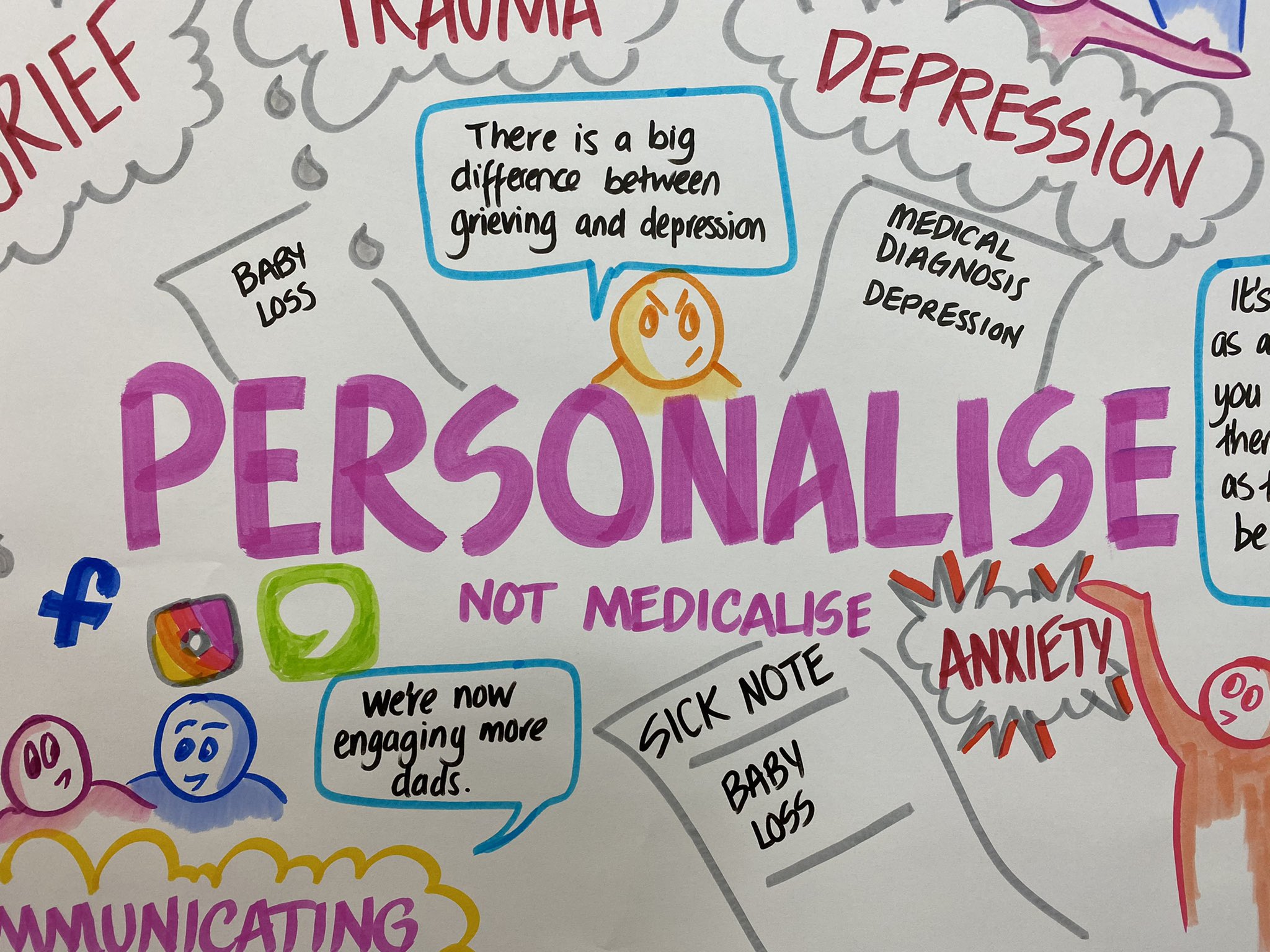
It was very moving to hear Deb talk about her experience of losing two babies before she went on to have healthy children, now teenagers. All birth stories are important. Hearing Deb remembering so clearly the things that made her experience better or worse, just as vibrantly as a mum talking about a very recent birth experience, brings home just how important things such as language, compassion, ‘personalise rather than medicalise’, and the other key themes of our #MatExp work really are.
Whose Shoes is constantly evolving. It is all crowdsourced by real people and their experiences.
Would you want to hear a group of student medics standing at the end of your bed, referring to you as ‘an interesting case’, as you come to terms with the loss of your child?
Would you want to receive a stark letter telling you not to get pregnant again until you come into the hospital to discuss your case … especially if you are already pregnant?
It is fantastic that we have been able to suggest practical solutions, such as the example set by Leigh Kendall, working with Kingston Hospital and St George’s, where sadly her baby son Hugo lived and died, to write more empathetic letters to bereaved parents. Please check out #HugosLegacy.
Catherine MacLennan, another bereaved mum, was similarly the catalyst for our innovative work around second trimester loss, which is sadly an area of care that is missed out from many ‘pathways’.
I am always in awe of how many bereaved parents use their grief to create something so positive.
We had the privilege of welcoming about 15 passionate bereaved parents/ couples in Gloucestershire, reaching out to help others. Many of them spoke about special people who had helped them along the way – “life savers” is a word frequently used. It reminded me of Catherine’s ‘special people’ poem.
Catherine’s ‘Special People poem’ reaching paramedics at London Ambulance Service
Something that I found particularly moving in our Gloucestershire event, was a mother talking about how, when her baby was sadly stillborn, she had made small matching dolls, one to place inside the child’s coffin and one to hang on the Christmas tree as a symbol of hope and for any subsequent children to enjoy and get to know and love their sibling.
I love the connections. 💜 The potential connections. 💜
I think my ‘goosebumps moment’ was the bereaved mum who’d made paired dolls. One for the baby’s coffin; one for perpetuity on the 🎄
We had some fantastic conversations around how best to help people remember their babies and how this might change according to the stage of pregnancy at which the loss occurred.
I have been able to follow this up, as part of my own personal pledge, by linking wonderful peer support people doing great work in this area.
Gill Phillips linking Lauraine, founder of ‘Shine’ and Leanne , founder of ‘By Your Side’.
Watch this space for further links between Lauraine Cheesman (Shine, Gloucs) and Leanne Howlett (By Your Side, Warwickshire)! I really love making these links!
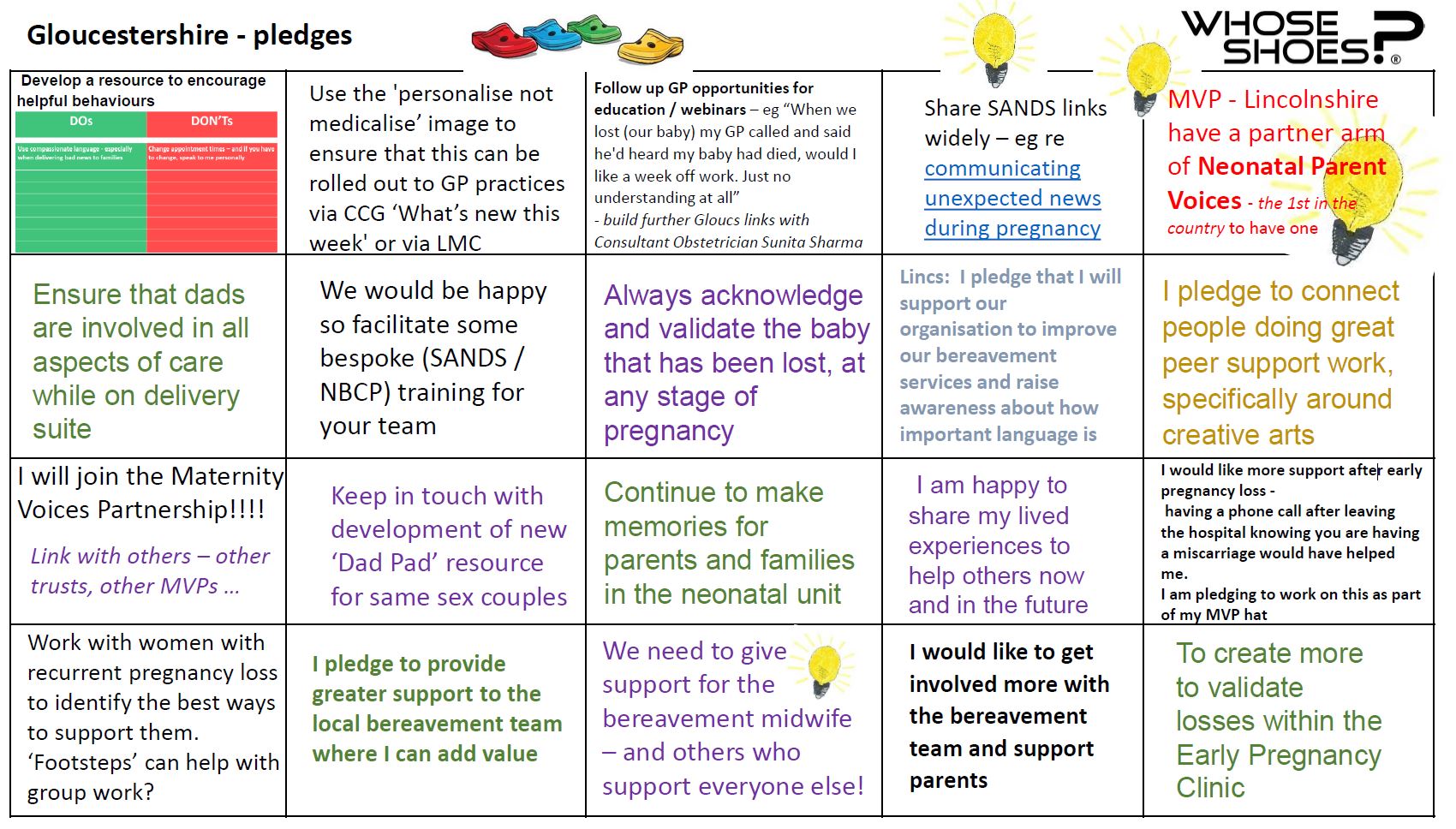
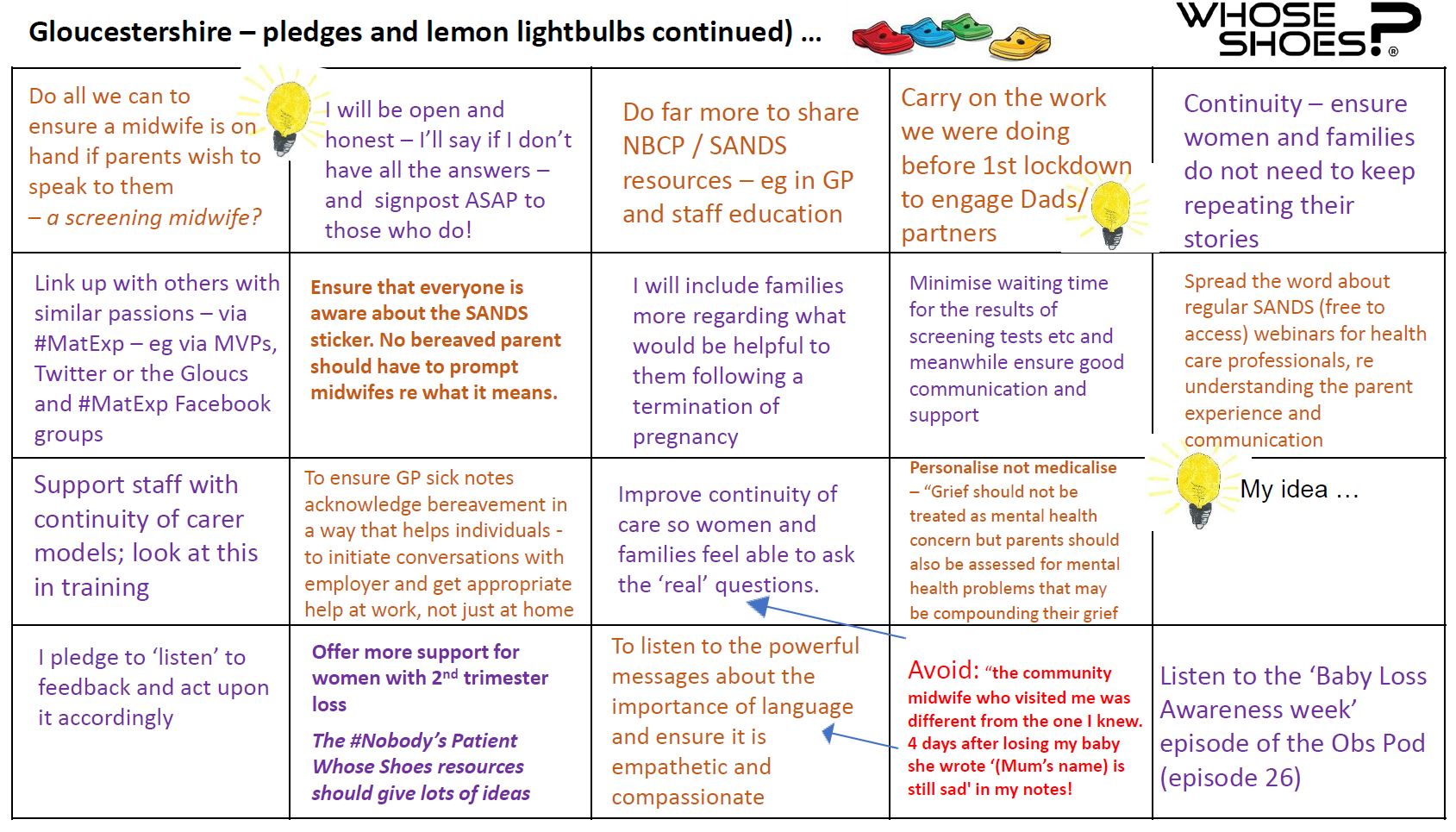
There were so many thought-provoking conversations, sparking the ‘lemon lightbulbs’ that stay with people and change practice.
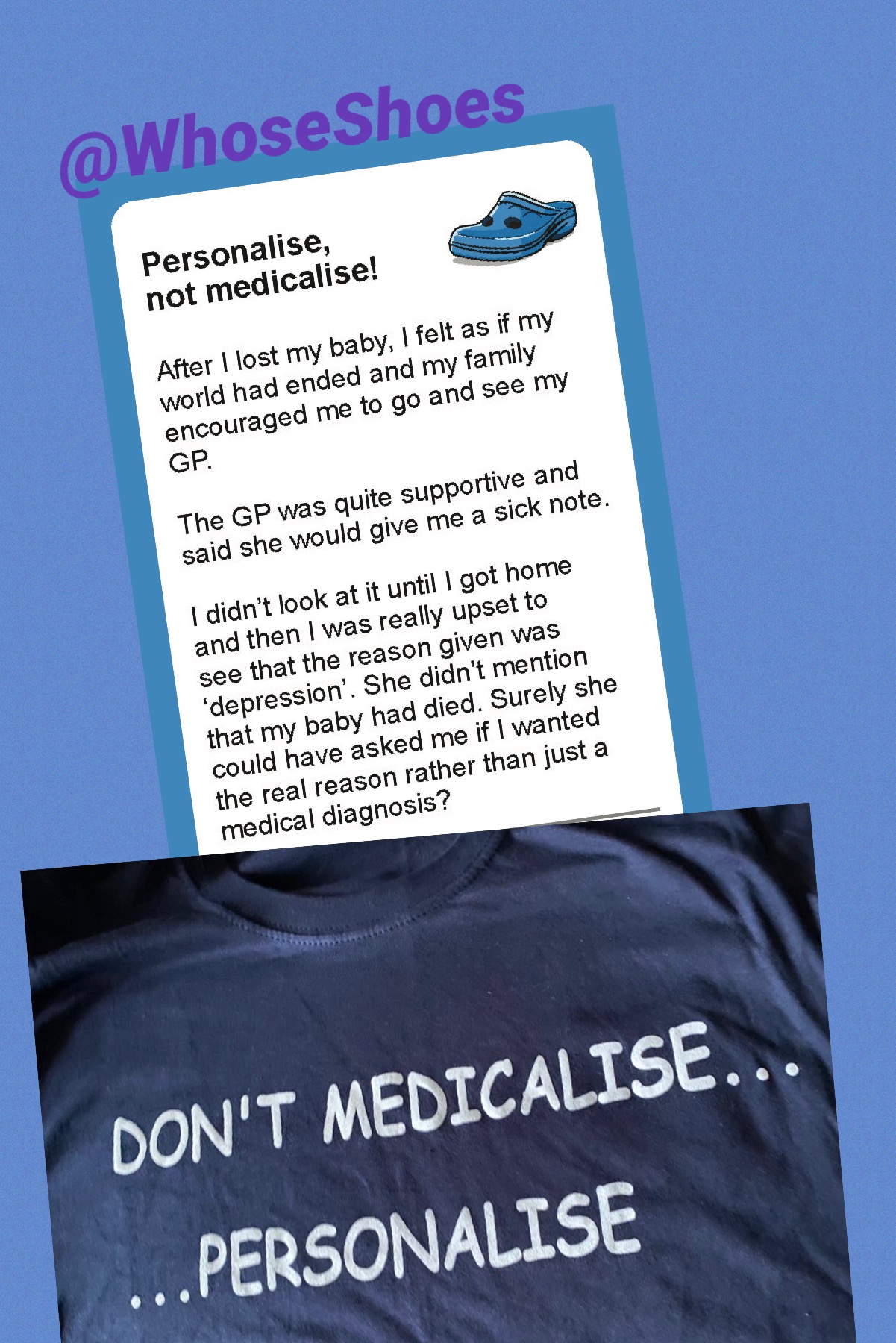
Would you want the doctor’s comment on your sicknote to simply say ‘Depression’ when you have just lost your child, without consulting you?
How would you feel having to handle this when you talk to your employer, sometimes without maternity leave if your pregnancy ends before 24 weeks?
These are just a small sample of the situations people are regularly facing.
Conversely, we heard how staff are generally extremely compassionate, and what a difference this can make, including giving people the courage to get pregnant again and try for ‘that happy ending’.
As always, we used a variety of scenarios and poems to generate the conversations to explore people’s experiences and how services and support could be improved. Bereavement midwife, Nikki Dobson proved to be a superstar. She and her colleagues had put in so much time to do a gap analysis, identifying areas where feedback suggested improvements could be made.
Thanks Dawn. It was a great planning meeting yesterday. Attention to detail in selecting scenarios & poems that match to the in-depth gap analysis Nikki did. These sessions are all about careful planning, true listening and working together towards real outcomes. 👍🏼 #WhoseShoespic.twitter.com/7gEdH7gp0Y
We wanted to get the most out of the opportunity afforded by bringing all these wonderful people from different perspectives together. The team had identified key themes and we selected the most relevant Whose Shoes scenarios accordingly, including:
• Some areas in fetal loss / medicine identified as needing improvement • Care after discharge • Delivery suite gap analysis • Antenatal screening – support for families in future pregnancies • Ultrasound • GPs • Supporting dads and partners
These are the visuals from the record today, recognising that support for dads and partners is different from the support for mothers #matexppic.twitter.com/avp0FAyj9N
Nikki writes wonderful poems and she generously read two of them live during our session. We have always used poems as a way of connecting with people differently in our WhoseShoes sessions.
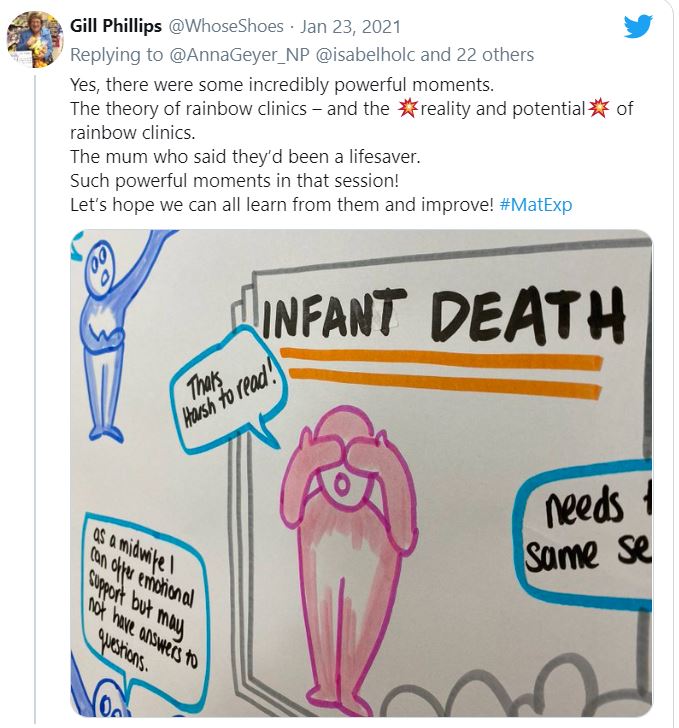
As always, Anna’s images were superb – and all the more so, being able to capture the conversations live during the session, just as we do ‘in the room’. Sometimes we have the opportunity of a visual learning synthesis too, but each event is different.
It is totally draining facilitating these online sessions but incredibly rewarding. The chat in the Zoom ‘chat room’ was phenomenal – full of wonderful insights, comments and useful links. The atmosphere was warm and supportive. We were able to ‘save’ the chat in all its richness, as another output from the session to feed into the continuing quality improvement journey.
The outcomes are extraordinary and just as powerful as any other events that we run.
And, of course, for all events the most important outcomes happen later – people following through and implementing their pledges, connecting, building the momentum for positive change.
Brilliant illustrations, really encompassing all the emotions and struggles surrounding baby loss
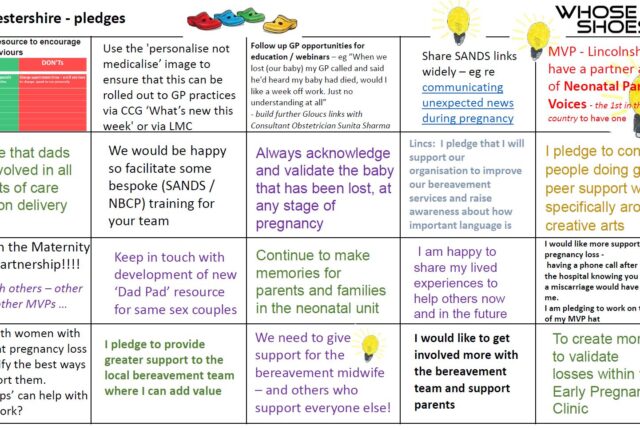
I collated as many of the pledges and specific improvement ideas from the session as I could. SO many. This does not mean that the bereavement care in Gloucestershire is poor. On the contrary, it means they are open to genuine coproduction, listening and finding out how they can make their service even better.
The praise – and indeed love – for Nikki, Dawn, the medical photographers, fetal medicine staff and many others was incredibly strong . I was moved by everyone’s determination to work together and support each other.
I am so grateful to have been a part of this today and excited to get to work on our pledges 💖
An amazing event today, such diverse conversations giving fantastically rich discussions and commitment to continue improving services for families who experienced bereavement through #babyloss#matexp#whoseshoespic.twitter.com/8hxYDvThcD
Kerri thank you and please join us to follow up on all our pledges we are all determined @daniellerees9@NikkiDobson1 to take forward the pledges and quality improvements from today
There seems to be a lot of interest in Whose Shoes around how we can better support parents and families suffering baby loss, building further on the various maternity projects we have done, which Colchester, Gloucestershire and about 70 other NHS trusts have used so powerfully in quality improvements.
Next stop, Lincolnshire? A few of their team joined the Gloucestershire session, which is always the best way to learn about Whose Shoes and build the networks. We’ve done some great work with Lincs before!
The energy is growing …
Since the Gloucestershire event, I have had several extraordinary opportunities to join conversations, hear different perspectives and ensure that our Whose Shoes material remains topical, authentic and able to spark the understanding that is needed.
Wonderful staff from the South-West neonatal teams came together to learn more about baby loss and its impact, and Nadia courageously shared her lived experience story, helping people understand the special grief and complexity of losing one or more babies in multiple pregnancy. I recommend this training highly to all involved in perinatal care.
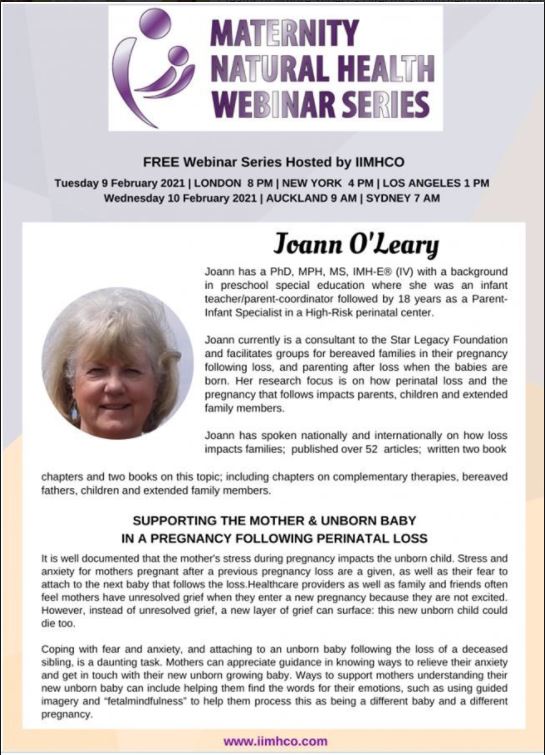
I also joined a webinar hosted by Kathy Fray in New Zealand, with guest speaker Joann O’Leary talking with huge insight about pregnancy after loss, another complex ‘taboo’ topic which is not discussed enough.
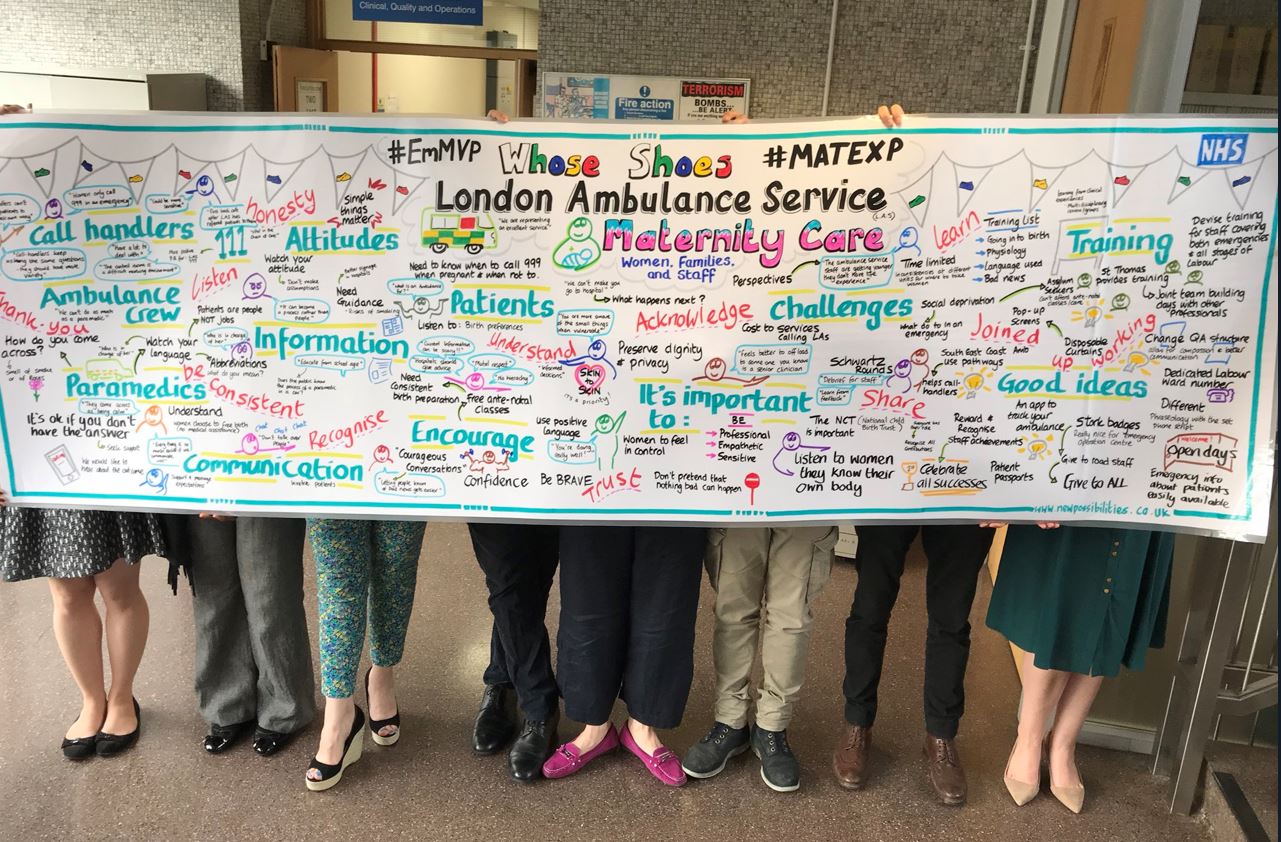
I am being asked about some of the ‘end of life care’ / palliative care work we have done in other areas – eg with London Ambulance Service. I am having some interesting conversations with People from NHS England / Improvement at the moment about how all of this work could be better supported.
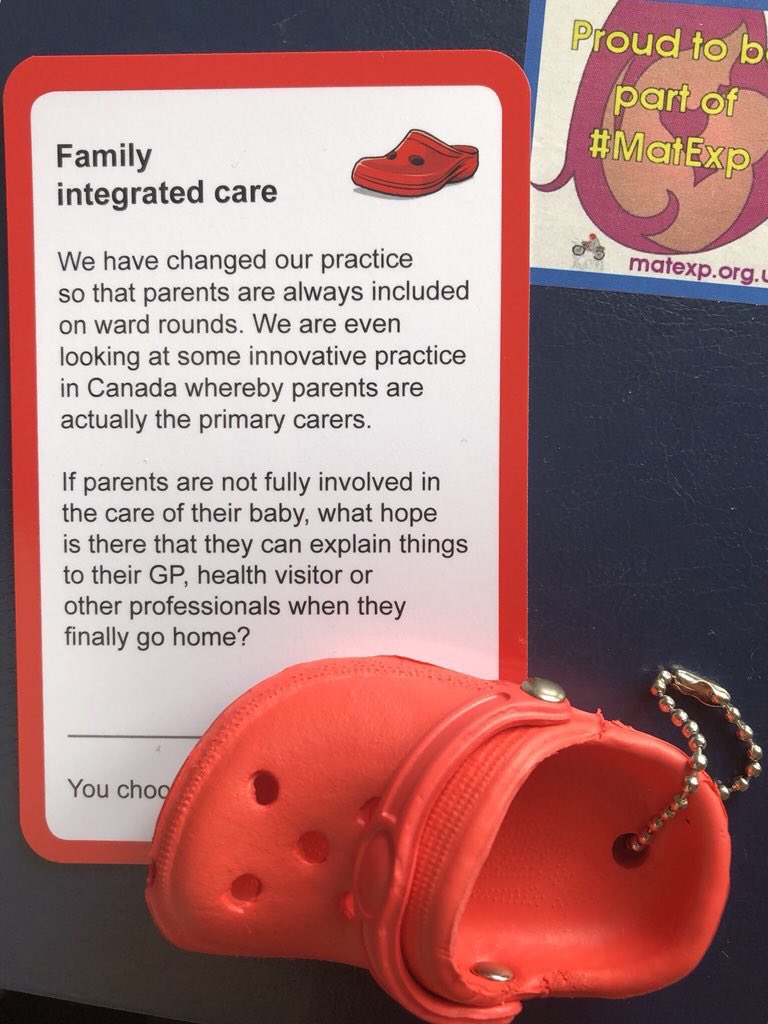
I am currently supporting a wonderful doctor, Nikki Crowley, to implement Family Integrated Care in a London hospital; the #NobodysPatient resources will be central to our collaboration. Networking is proving super important here, as some wonderful people come together to help.
And … latest news … we are currently looking at innovative ways to help people follow up Whose Shoes pledges, if things get ‘stuck’ in any way, using #LiberatingStructures. With thanks to Lyse Edwards. Contact me @WhoseShoes if you want to know more.
So, lots happening. But it is only be happening because PEOPLE are stepping forward to make a difference, which is hugely rewatding.
I will leave you with a fantastic quote from Nadia Peake, the bereaved mum of twin baby Raif, who stole the show at the South West Neonatal event.
“The situation is bad. The experience doesn’t have to be”
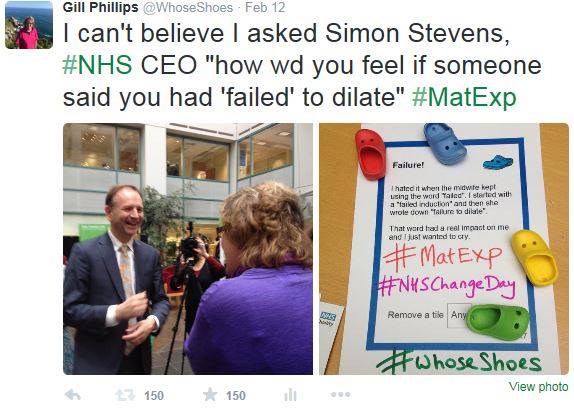
When I started thinking about women’s experience of maternity care five years ago, some of my colleagues were rather dubious; ‘safety first’ was their view: why would I bother about the ‘fluff’ of personalisation? Experience can sometimes be seen as a midwifery issue rather than relevant to doctors. I wrote a blog to try and dispel this idea https://matexp.org.uk/birth-trauma/safety-experience-or-both/ .
In contrast, I have had wonderful support from RCOG, almost from the beginning first meeting with then President David Richmond in 2015.
David Richmond running a patient experience breakout session at the launch of ‘Better Births’ at the Oval – Sarah Winfield says Whose Shoes works! And who is out???Flo’s first #MatExp visit to RCOG to meet with David Richmond and tell him about #MatExp Whose Shoes coproduction work. A symbolic little (shoe) step along the way.
RCOG firmly believe in the ethos of working with women collaboratively and making sure women’s views are front and centre of everything we do in the profession. Despite this I have worried that the O&G doctors who attend our workshops or hear me speak are those that already practice in this way, ‘preaching to the converted’ one might say. I have wondered how to bring #MatExp and co production to a wider audience and start to influence our more sceptical colleagues. I have long thought the best way would be to get on the agenda of one of the RCOG mandatory training courses.
The annual ‘Management of the Labour ward’ course seemed like a great starting point so with the help of Louise Page, BICS president and Alison Wright & Kate Brian of RCOG women’s network, I managed to get agreement to run a Whose Shoes co-production session one evening in May. All the best #MatExp sessions are collaborative, so I drafted in a few friends from National Maternity Voices as well as fellow obstetric consultants who are actively using co production.
It was also brilliant to be joined by Nicola from Positive About Down Syndrome (PADS.) My aims were very simple, I wanted to give people a taste of co-production, challenge their assumptions and encourage them to link with their Maternity Voices Partnership or other parents’ groups and take the idea of co-production back to their workplace. I gave a brief introduction and invited people to play Whose Shoes, facilitated by my willing volunteers.
Setting up the room ready for our Whose Shoes? co-production session
Running as an additional session at the end of a long day, it wasn’t surprising that we had a relatively small number attend our session, with 24 completing feedback forms. The feedback we had was incredibly positive.
Not only did 75% of attendees say the session had impacted on the way they will work with women and families in the future but in addition the majority of attendees had no previous experience of co-production so we definitely reached a new audience.
I am really hoping that the success of the session means that this is just the start. The new curriculum seems like a brilliant opportunity with much more focus on the softer skills of communication and treating women holistically rather than seeing them as a medical condition or operative procedures to tick off in a log book.
RCOG world congress in June again demonstrated firm commitment from the college with lived experience being threaded through the three-day programme, culminating in a co-produced presentation by Emma Crookes (RCOG women’s network) and myself on the final day. You can view it here:
I have recently joined RCOG women’s network as a clinical representative and have been delighted to see the depth and breadth of their work. Women’s voices have become well embedded throughout RCOG work everything from guidelines to workforce, examinations and genomics. With their help I am hoping this heralds a new era with co-production, personalisation and informed choice central to the care we provide.
As more and more people join the fabulous #MatExp community, they may not know the origins of #MatExp, co-founded by Florence Wilcock and Gill Phillips in 2014.
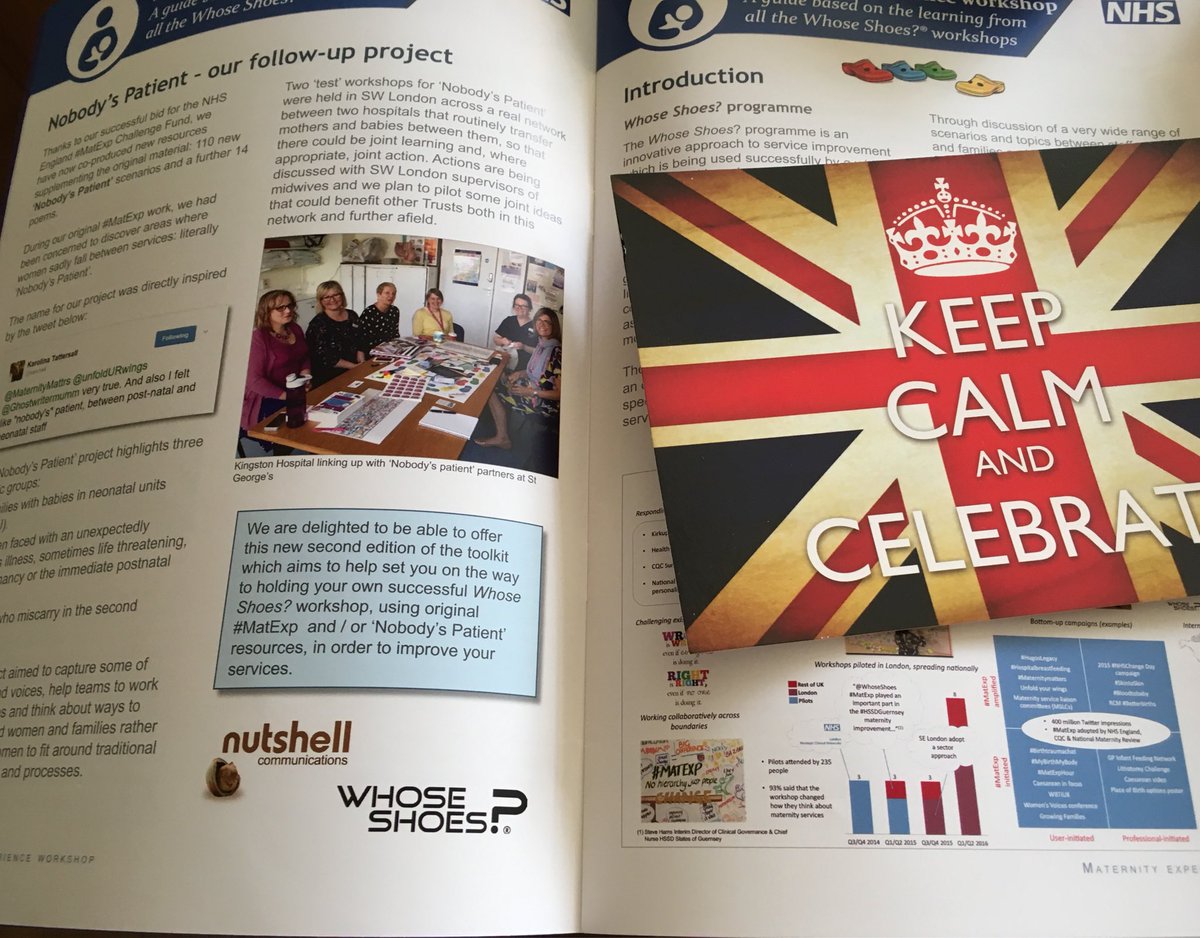
People may not realise that we published the original Whose Shoes? scenarios and poems at the beginning of 2015, before maternity hit the national spotlight and the national maternity review was announced.
The resources were used at all the national maternity review listening events and helped enrich and shape the conversations that led to ‘Better Births’.
People ask for ‘evidence’ of what #MatExp Whose Shoes? has achieved…
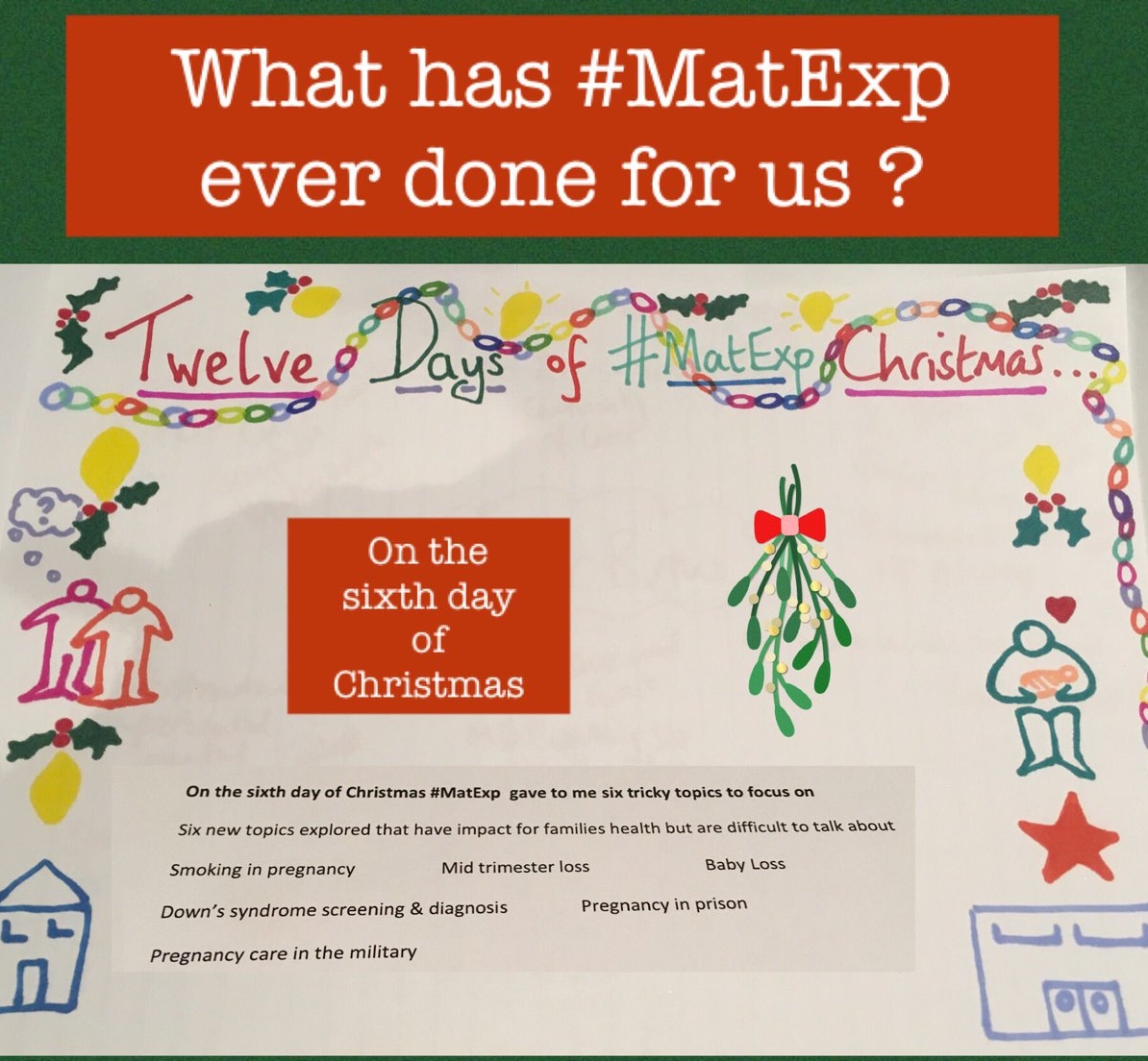
And so we bring you our #MatExp 12 Days of Christmas, published in the lead up to Christmas 2018, summarising some of the biggest achievements and outcomes to date. We have helped serve as catalysts. The big achievements have only happened because fantastic people have come together and found that individually we can all make a difference, but TOGETHER we can ‘be the change’.
Each of these ‘things that #MatExp brought us’ has a story behind it; sometimes a big one. Who knows, one day we might get round to writing THAT book. But in the meantime, this is all we have time for. So if you want to know more, please join #MatExp. And most importantly, keep adding to the story. These small or large individual contributions are how positive change will keep happening.
Remember those heart values – all of us working together to improve maternity care. Thank you!
#MindNBody And, new for 2019, our #MindNBody campaign – using new crowdsourced Whose Shoes? scenarios and poems to spark crucial conversations around perinatal mental health. A holistic approach, looking to improve the experiences of women and families, including prevention and early intervention. The resources were launched at the Royal College of Obstetricians and Gynaecologists in December 2018 and a diverse mix of people involved in the project made a two minute video for the days of Advent, which are compiled into a single film here:
In December 2018, we were proud to launch our new #MindNBody Whose Shoes? resources – the third in our series of major #MatExp projects to improve maternity care and help people to focus on a holistic ‘Mind N Body’ approach to maternity experience.
The whole thing is crowdsourced, with scenarios and poems contributed about a very large wide range of issues, and from all perspectives.
At the last minute, we got the idea to crowdsource videos from some of the people who’d been involved, as a #MindNBodyAdvent series. Take a look at the hashtag on Twitter . It was very organic and came together better than I dared hope , with lots of fantastic people volunteering to join in .
Here we have collected them into a single video and I hope they give you a feel of the depth and variety of the project.
The new resources are currently going out to over 50 NHS trusts and we hope will support conversations to improve experiences of women and families everywhere .
A Happy New Year to all – hoping 2019 will be another year of positive, action-focused #MatExp change and looking forward to working with everyone to get the most out of the brand new material.
I had an idea for #NHS #FabChange70. I decided I would collect 70 different things that have happened as a result of #MatExp #WhoseShoes and share one a day until the official start date for the #FabChange70 on 17 October.
@MrWhoseShoes rolled his eyes. He knows that these things are in danger of taking over my life (and therefore our lives!) So I promised to keep it simple.
Ideally, I could perhaps have done something sophisticated, crowdsourced the best 70 ideas (there are plenty to choose from!), got different contributors to write a blog, or otherwise tell their story, every day for 70 days… 70 days is a long time and I really don’t have the time.
Apologies in advance if I do not include something important, as I’m bound to miss lots of good stuff! If there is anything you are desperate for me to be include, please get in touch and we can build it in.
So let’s keep it simple. Let’s have some fun. 70 fab #MatExp things And here’s the first one…
#StopNCelebrate
And what could be better to start with than #StopNCelebrate? Like most of our best stuff, this was a spontaneous idea that came from one of our #MatExp #WhoseShoes workshops. So the aim is: 70 things that come to mind that give you a flavour of the sorts of stuff we get up to through – culminating in a Steller story that pulls it all together. Steller stories only allowed 75 pages. Therefore only one page per idea. That has to be simple! Wish me luck!
Here is the story of the workshop that led to #StopNCelebrate.
And here is the story of how #StopNCelebrate caught fire! Well done … WARWICK HOSPITAL!!
Important insights by Florence Wilcock, consultant obstetrician at Kingston Hospital and co-founder of #MatExp, as we celebrate the 70th birthday of the NHS today,
5 July 2018.
One cannot open a newspaper, listen to the radio or turn on the TV without a reminder that today the NHS turns 70. For many of us this means that we have no recollection of not having had health care free at the point of use, so perhaps we sometimes take it for granted. The sentiment of being able to do what I feel is right for my patients regardless of cost and without personal gain has always been of central importance to my desire to practice medicine. As we approach the celebrations I’ve been feeling a little despondent, it’s hard to shout and cheer when dealing simultaneously with unprecedented scrutiny of quality and finance and a level of bureaucratic oversight can feel stifling.
Therefore as the NHS turns 70 & I celebrate having worked in the NHS for 25yr here are a few of my positive reflections on NHS maternity care.
The NHS trained me; don’t forget that not only does the NHS treat and care for patients, it provides clinical training for the many doctors , midwives and associated healthcare professionals of the future. The babies born when I was training as a medical student would now be 26yrs old; if I hadn’t witnessed and helped at those births I would not have been inspired to be an obstetrician helping and caring for women now.
Over the years the NHS has also contributed to specialist training of many overseas doctors some of whom now practice here, but many of whom return home and benefit women and families across the globe.
Although British I was born in Brussels and my parents tell the story of arriving at the hospital with my mother in the late stages of labour and my father having to confirm his ability to pay before they started to look after her. I cannot imagine looking after someone in these circumstances. I have seen maternity bills on Twitter reaching $20000 from the USA and have talked to people when I travel abroad about their difficulties in affording basic antenatal and intrapartum care; in this country we do not give this a thought.
We have first rate neonatal care so that babies born prematurely have the best chance of survival, I know mothers in other countries who have not been so lucky, our babies do not die through lack of equipment such as an incubator or ventilator.
When we celebrate all those babies born in the NHS over 70 years, we must not devalue those of us who were not. Many excellent work colleagues and families using maternity service were not born here but do contribute to and deserve the excellent maternity care that the NHS can provide.
Although the NHS can sometimes seem a huge faceless organisation cited as wasteful and cumbersome, I know it is full of the most dedicated, hard working people and that day in day out these people are trying to make a difference as best they can in challenging circumstances.
During my work in Maternity experience #MatExp I have found many like-minded maternity health professionals whowant to work in genuine partnership with women and families and being open and honest about our limitations and co-producing solutions.
So as we celebrate the NHS 70th birthday, let us try and build a foundation for the next 70 years of maternity care that we can be proud of.
On Monday, to begin #ExpOfCare week, we had an insightful blog from Dr Sarah Winfield reflecting on her experience of taking part in the ‘Lithotomy Challenge’. And today, to end #ExpOfCare week, another #FabObs, Dr Florence Wilcock – the originator of the #LithotomyChallenge and co-founder of #MatExp – tells us all about Caesarean sections and what really happens…
Dr Florence Wilcock
As we come to the end of #ExpOfCare week, I would like to share a blog about Caesarean sections, to demystify the birth that mothers and partners may unexpectedly experience. I originally wrote this blog at the request of Milli Hill & the positive birth movement in October 2016 , subsequently this has been included as a contribution to Milli’s book ‘The Positive Birth Book’ published 16th March 2016.
Why do we need to talk about Caesarean sections?
Unfortunately, sometimes people can be prone to making value judgements about different types of birth. One of the most common examples is vaginal birth = good and Caesarean section = bad. The truth is that in the UK current statistics show 25% of women will give birth by Caesarean section, 10% planned so called ‘elective’ and 15% unplanned ‘emergency’. We can argue these rates back and forth; we can aspire to improve care and change these facts, but for the moment given that 1in 4 women will meet their baby in the operating theatre it is vital that we talk openly about this experience and how it can be a positive, emotional & fulfilling birth for each new family.
Even in an unexpected ‘emergency’ there are still choices to be made. Nice guidance on Caesarean section CG132 section 1.4.3.4 recommends 4 categories of urgency; only category 1, the most urgent suggests delivery within 30mins. Far more common is the ‘emergency’ caesarean category 2, delivery within 75mins of decision making. This gives a woman time to express contingency birth preferences and ensure that even if she did not plan a caesarean birth it remains a calm and positive start for her and her baby. Skin to skin in theatre, optimal cord clamping, birth partner announcing the sex of the baby, choice of music are all possible. I would love to say these are all standard in every hospital but unfortunately that wouldn’t yet be true, however the more women know and ask, the more these will become universally accepted. As I often say ‘Wrong is wrong even if everybody is doing it and right is right even if nobody is doing it’. I wish you all an interesting and positive month discussing Caesarean birth and would like thank Milli for inviting me to contribute & become part of it. If you want to know more about how I am working to try and improve maternity services do check out matexp.org.uk
Caesarean Section a theatre experience & Who is who in the operating theatre?
The majority of caesarean sections in the UK will be done under a spinal anaesthetic, that is numb from the nipples downwards. It’s a peculiar feeling as one can feel touch but not pain. It means that women will be awake and aware of people milling around them which can be daunting but it also means they are awake and ready to meet their new baby. Lying on the operating table we tilt women slightly to their left to keep the bump of the baby off the major blood vessels, this prevents dizziness from low blood pressure. If you lie on the operating table in the maternity theatres at my Trust you will look up and find butterflies & cherry blossom on the ceiling, something nice to focus on while you wait for your baby to arrive. I know this is unusual & we are lucky but there is nothing to stop you tucking your favourite picture or photo in your birthing bag so that you have something familiar and relaxing to look at.
It might seem odd that at the start everyone in the theatre will introduce themselves to one another. It isn’t that we have never met but its start of the World Health Organisation (WHO) safety checklist. There is a special checklist just for maternity theatres and it is routine to start by checking simple information such as the woman’s name and date of birth and move onto clinical issues and equipment and it is all aimed at making the experience as safe as possible. So, who are all these people around you and what are their roles, why are there so many people there?
Anaesthetist: At least one sometime two; these are doctors who will administer the anaesthetic ad monitor you closely during the surgery. They will be standing just by your head and often chat to you and reassure you as the operation progresses.
Operating Department Practitioner (ODP): at least one; their role is to assist the anaesthetist, getting & checking the required drugs, drips or equipment, the anaesthetist cannot work without one being present.
Obstetricians: at least two; one will be performing the Caesarean section (the surgeon) the other will be assisting (the assistant) e.g. cutting stiches, holding instruments.
Midwife: At least one; to support the woman and help her with her newborn baby when it arrives
Scrub nurse or midwife: At least one; To check, count all needles, stiches and instruments and to hand them to the surgeon when needed.
Midwifery assistant or runner: This person double checks the swab and instrument count with the scrub midwife or nurse and ‘runs’ to get any additional equipment required as they are not ‘scrubbed up’ so can go in & out of theatre to fetch things.
Paediatrician: asked to attend any ‘emergency’ situation or if there are known concerns about the baby.
So, you see in theatre there is a minimum of seven people caring for any woman all with specific tasks to perform, any complication may result in us calling in extra members of the team.
So back to the woman, she will be on the operating table with her birth partner by her side and the anaesthetist and ODP close at hand. She can often choose the music she would like her baby to be born to. The anaesthetist needs to monitor her heart with sticky labels but these can be put on her back and her gown left loose leaving her chest free and ready for skin to skin with her baby. A sterile drape will be placed over her bump and this is usually used to make a ‘screen’ so that the woman doesn’t see and surgery she doesn’t wish to see however usually we drop this when the baby is ready to be born.
Many hospitals are starting to explore options of optimal cord clamping (waiting to clamp the cord) and passing the baby straight to the mother if the baby is in good condition. These can be done but need to be thought through so as not to contaminate the sterile surgical area, and the surgeon needs to be confident no harm such as excessive bleeding from the womb is happening whilst these things occur. Surgical lights need to be on so the surgeon can see clearly and operate safely but I know one anaesthetist who works in a hospital where the rest of the theatre lights can be dimmed. The mum and new baby can be enjoying skin to skin whilst the rest of the operation proceeds. Weighing and checking babies can be also done at this time but also can be done later on.
Traditionally if we operate with women under a general anaesthetic (asleep) her birth partner has not been in in theatre as their role is to support the woman. Recently on several occasions I have challenged this so that a baby is welcomed to the world with at least one of its family present and awake rather than by a group of strangers caring for the unconscious mother. There are safety considerations to be talked through for this to be successful but it is possible. However, kind and caring staff are, they are no replacement for a birth partner whom the mother has chosen to support her in the intimacy of birth.
I hope I have given you a brief glimpse in to life in a maternity theatre. As an obstetrician, I am privileged to help bring many women and babies together for those special first moments. The emotions are always different for me: sometimes it is a couple I know very well and have bonded with over months or years, sometimes a woman I have only just met who has had to put her absolute trust in me immediately. The theatre atmosphere can range from almost party like jollity to quiet intimacy. Every birth is different; each birth is extremely special just as much as the births that happen in a less clinical environment and each birth will stay with that woman forever.
We are very honoured to begin #ExpOfCare week with a bang, publishing this insightful blog by Dr Sarah Winfield. We have connected with Sarah through the excellent ongoing #MatExp work at Leeds Teaching Hospitals NHS Trust, following the exciting Whose Shoes? workshop last summer. Part of the work in Leeds involves a different #MatExp challenge each month… and January 2017 was ‘lithotomy challenge’ month!
Sarah wrote this a while ago but we held it back to publish here as #ExpOfCare is such an important initiative and one which is central to #MatExp. We are very grateful to Sarah not only for taking the time to do the challenge, but more importantly to reflect so openly on the experience and share with us here…
The #LithotomyChallenge is a term coined by one of my Obstetric colleagues in Kingston, Dr Flo Wilcock, who wanted to put herself in the position of a patient in lithotomy for an hour and to describe the experience. As part of #MatExp and to raise awareness of it’s existence and philosophy, I wanted to do the same. So I did on #NHSDoAthonDay at the start of January 2017. Here is how I got started.
I used to be sceptical about twitter until my tech-loving husband persuaded me to dust the cobwebs off my twitter account @winners352 (set up tentatively a while ago). David is a consultant in Education and assured me that performing CPR on my twitter account would not only be beneficial for my CPD, but would put me in touch with like-minded people, allow me to tweet the odd journal article, and would help me to raise the profile of the unit that I work in. I wasn’t ‘sold’ but I am an optimist and thought that I should give it a go.
So I changed my profile picture, tried to compose a sassy yet professional catch line and I started to browse for people and things that may interest me. Initially I retweeted posts that would not cause any controversy for my digital footprint or reputation as a member of the medical community, but then I worked out that if people put their opinions out there for all to see, then this provokes engagement and discussion. This conversation would then draw others in. Then information begins to flow, more people ‘follow’ and before you know it, there are people from all over the world tapping in to see what this is all about. Amazing. But also slightly scary.
Of course, I appreciate that there are downsides to having a twitter presence, but this is where the world is going now. I recall an article written for the Health Service Journal by Roy Lilley about STPs (Sustainability Transformation Plans). In this article, to paraphrase, he said that STPs are happening and are not going away, so you can be in the cast or the audience. It’s your choice. I think that the same applies to social media and twitter. So, I made the decision to learn more and make it work for me. This was at the beginning of October 2016.
Through twitter I made contact with Gill Phillips (@WhoseShoes) and Flo Wilcock (@FWmaternitykhft) who are the founders of #MatExp, and it turned out that I had actually met one of this duo before!
As well as being a Consultant Obstetrician with an interest in maternal medicine, I am also the Clinical Lead for maternity services for the Yorkshire and the Humber Clinical Network. This role took me to an event at the Kia Oval in London in July 2016 to discuss implementation of ‘Better Births’ (the National Maternity Review) in each network patch. There were a series of workshops and in one I joined in with a discussion about the “Whose Shoes” event that had been held in Leeds earlier in the year. I did not realise it at the time (probably because I was not on twitter at that point!) but Gill Phillips was one of the facilitators of that group. Professor Cathy Warwick and Mr David Richmond were the other facilitators.
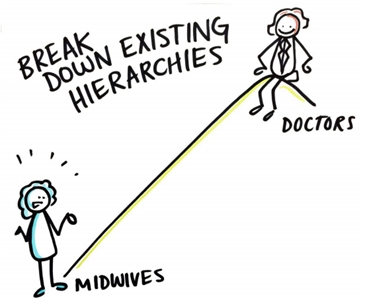
While I had not been able to attend the Leeds Whose Shoes event itself, our LTHT strategy midwife, Sarah Bennett, was very much involved. At the event a cartoonist, Tom Bailey, recorded patients’ views and the conversations taking place. These were very thought provoking and I have to admit that one image in particular made me stop and think. It was of a doctor standing at the top of a hill pointing down to a midwife at the bottom of the hill. It was not particularly complimentary to us as doctors.
None of us set out to make patients and midwives feel like this but with the language we use, the information we need to get across and our communication skills in general, there was clearly an issue. This made me feel uncomfortable (and perhaps a tad indignant, if I am being honest) and I know that a few of my colleagues felt the same as me.
What happened though was that these images stimulated discussion and debate amongst the maternity staff members. While there might have been levels of disagreement about the images and what they portrayed us to be as medical and midwifery professionals, they were ‘real’ views of and we had to reflect here. Importantly these conversations were a starting point to encourage us to look at how we work on a day-today basis, the language we use with patients and each other, how we conduct ward rounds on the delivery suite and the whole experience for any woman and her family using our maternity service.
In other words, we had a platform from which to share our opinions about the maternity experience of patients in Leeds across both sides of the city.
Leeds is a busy tertiary unit. We have around over 10,000 deliveries a year between Leeds General Infirmary (LGI) and St James’s Hospital (SJUH) and we don’t often get to do sit down with our colleagues, whose opinions we genuinely value, and engage in a dialogue about patient experience. But here we were, and I felt like this was a good start.
I spoke about this experience in positive terms at the Kia event and Gill then made contact with me through twitter a few months later. A fortuitous connection for me and, I hope, for her too. I also ‘met’ Flo through Gill on twitter, and the rest has followed.
So who are Gill and Flo and what is #MatExp?
Gill, the creator of the award-winning Whose Shoes?® concept and tools, has a genuine passion and unsurpassed energy for “looking at issues from different perspectives and getting people to talk together as equals and come up with imaginative solutions”. She is also a mum of three ‘now grown up’ children.
Her website http://nutshellcomms.co.uk/gill-phillips-and-the-origins-of-whose-shoes/ is an inspirational working ode to her warm, inclusive and collaborative style. Gill’s passion for helping others is obvious to see and she takes people with her. This is one of the many reasons why she has been quoted by the Health Service Journal as one of the 50 most influential women of the year.
Florence (Flo) Wilcock is a Consultant Obstetrician at Kingston (and mum of two) and, inspired by Gill’s WhoseShoes concept, was keen to use this to improve maternity services and more. Flo is similarly an inspirational force and counts the RCOG and its former president David Richmond as her supporters, amongst many others. She joined forces with Gill and the #MatExp campaign was born.
The #MatExp website is a vibrant, colourful, positive and proactive resource and I would advise anyone working with women and their families. The best explanation of #MatExp is the one from their website, so in their own words:
“#MatExp is a powerful grassroots campaign using the Whose Shoes?® approach to identify and share best practice across the nation’s maternity services.
Then ensued a flurry of tweets between me, Gill, Flo and other #MatExp supporters and I was overwhelmed by the helpful, collaborative and go-getting approach. They are incredibly supportive to anyone on twitter who shows an interest in improving patient and family experience in maternity services.
As my knowledge grew about #MatExp and I had further twitter conversations with Gill, Flo and others, I read a piece by Flo that she wrote about her taking part in a #Lithotomychallenge. The piece is here and Flo explains:
“For NHS change day I wanted something that made a statement that said “#MatExp has arrived, take notice, we are improving maternity experience, get involved!” I couldn’t quite think of the right action until I saw a twitter exchange with Damian Roland back in December and watched a video where he described his spinal board challenge from NHS Change day, 2014. I had a light bulb moment thinking what would be the maternity equivalent? Lithotomy!”
Taking Flo’s lead and transporting #MatExp to Leeds, I thought that a #LithotomyChallenge would be easy for me to set up and would put me in a patient’s shoes (goodness knows the amount of times in my career that I have put a patient in the lithotomy position for an instrumental delivery, a FBS, a perineal repair..) for a short while. I have two daughters, both born by caesarean section, so I had no experience of this, let alone with contractions, CTG leads, an epidural, a syntocinon drip etc.
I chose Wednesday 11 January 2017 as the morning I would do it. This was #NHSDoAthonDay and it seemed appropriate.
In the run up to the day, Sarah and I told people what I was going to do through the strategy newsletter, facebook, twitter and word of mouth. People asked why and asked what #MatExp was. There was also an interesting spectrum of opinion about my desire to do the #Lithotomy Challenge, ranging from people thinking that I was ‘patronising’ my patients and colleagues to others congratulating me for taking the initiative to do something different.
On the day of the challenge I put my hospital gown on, strapped the CTG leads to my abdomen and Sarah fixed an IV line to hand with tape and helped me up onto the delivery bed in Room 10 on LGI delivery suite. Then Sarah left to go across the city to St.James’ hospital where the midwives there were waiting for her to set them up with the #Lithotomychallenge too. I was by myself in the room. In lithotomy position.
I felt undignified and vulnerable. I also hoped that nobody would walk through the door, but they did. In groups, in pairs, alone. Mostly midwives. Each time I cringed as the door opened and I realised that the level of the bed meant that my bottom end was at their eye level. I was in leggings and a sheet. I can’t imagine the indignity and embarrassment for a woman of being ‘al fresco’ when someone comes into the room in that situation.
Then I noticed something that I hadn’t before; there was no ‘privacy curtain’ over the door. I now realise that this curtain is a feature of the delivery rooms at St.James’ hospital across the city and in every other maternity unit I can recall having worked in before. Such a simple thing would make a huge difference.
Then the surroundings really began to jump out at me. This room had magnolia walls, a light socket that was hanging off (previously an uplighter), holes and scuffs in the walls and nothing that I would describe as comforting, pleasant or homely. When you sit in a room for over an hour, these details are very obvious. I have been in this room many times during ward rounds, to deliver babies etc. and I had never noticed what an uninspiring and depressing environment it is.
Would I have enjoyed my birth experience in this room? Definitely not. Does it convey an impression of the warmth, skills, knowledge, team spirit and professionalism of the delivery suite staff that I know exists? No it does not. But a woman and her family have this room as the starting point on their personal, special and much anticipated journey to give birth to their precious baby so how is it going to set them up for a positive birth experience? It don’t think it will.
Then something unexpected happened. I felt really cross with this room, if it’s possible to be annoyed with a ‘space’. I know how hard the team work to look after women and their families, so why should the woman and us as the team, with our training, skills, compassion, knowledge and tertiary centre reputation be let down by awful facilities? All women should have a pleasant environment to have their baby. It’s very simple. Some paint, some wall décor, good lighting, promptly repaired faults. The list is not long and is easily addressed. This was the first unexpected result for me of my #Lithotomychallenge and I have to say that it really touched a nerve.
The other unexpected result for me what that when people came in to see me they shared their own birth experiences (good and bad) as I sat there on the bed
with my legs ‘akimbo’. I found this moving because these are people who I have worked with for the last few years, who I chat with when I’m on-call and who I think I know quite well. I heard stories of a fantastic waterbirth, an awful induction, someone struggling to get pregnant plus more. You could say that the ‘barriers’ were down, but I would like to think that me doing this challenge provided an opportunity for people to start conversations with me and each other about their experiences as patients in the maternity service.
My final recollection added some humour to my experience. While I was talking to a group of student midwives (they appeared to be more embarrassed than me), one of our delivery suite domestic staff, who I know quite well, knocked on the door, walked in politely and without ceremony, gave me a glass of water and asked me for the keys to my office so that she could give it a clean while I was tied up! There was no pulling the wool over her eyes. I gave her the key and my thanks.
So, what did I get out of doing the #Lithotomy challenge? There are two things that stand out for me. The first is that I allowed myself to ‘feel’ from a patient’s perspective. I was prepared to give a bit of myself away and open up to the possibility that we may not communicate in a way that enhances a patient experience or consider the importance of the environment that we create to do this. I think that to change culture, the language we use and the way we view the patient experience we need to look closely at our individual practice and challenge our own behaviours and judgements. This is hard and not everyone will want to do this but I have found that doing the #LithotomyChallenge has led me to review my own beliefs and practices as an NHS worker for almost 20 years and this has been like taking a deep breath of fresh air.
As a doctor and a consultant I am familiar with pushing my boundaries professionally and clinically, but can I use any ‘influence’ that I have in a different way? Of course I can be an ‘opinion’, counsel patients, make management plans, perform difficult c-sections, chair regional meetings etc. but working towards improving patient experience may be regarded by some as a ‘fluffy’ goal. Very ‘touchy feely’ and not really hard-hitting or go-getting enough to warrant using precious consultant time in an already busy day where we are here to deliver a service and fulfill the objectives of our job plan/appraisal personal development portfolio. But sometimes it’s not until you experience the ‘other side’ and and allow yourself to ‘feel’, that you realise what needs to change. I now know that I would like to be more proactive in considering the whole patient experience when I am involved in any aspect of a consultation or a procedure.
The décor was the second thing. I have seen many articles and personal commentaries about the effect of surroundings on birth experience, and we already know that the environment during labour and delivery can have a profound effect on how patients ‘experience’ their care. After spending time in a room that has seen better days, I can believe it. Never underestimate the importance of surroundings and this challenge has highlighted that for me. I hope that this piece will result in privacy curtains being put up in each delivery room at LGI. This would make such a difference. But improving the delivery rooms in this unit is going to require funds. I regularly see healthcare workers and patients fundraising for their units and doing the #Lithotomychallenge to spurred me on to do this.
There is one final thing that the challenge has done. By writing this piece I have a voice. I have not asked permission and have not sought the ‘approval’ of anyone. I have just done it and have been supported by most of my colleagues, including Sarah B. I was nervous about doing the #LithotomyChallenge and had a sense of trepidation about what others would think, but I have enjoyed what the experience has brought and have been inspired by Flo and Gill, who have given me a masterclass in wholeheartedly and warmly welcoming others thoughts and diverse opinions. In their eyes no opinion is ‘wrong’ or ‘daft’. If disagreement arises then it is not to be feared or ridiculed. It can be used as the basis of a conversation to challenge the status quo and then move forwards.
“Change will not come if we wait for some other person or some other time. We are the ones we’ve been waiting for. We are the change that we seek” (Barack Obama).
Dr Sarah Winfield Consultant in Obstetrics with Special Interest in Maternal Medicine. Leeds Teaching Hospitals NHS Trust Yorkshire and the Humber Clinical Network Clinical Lead for Maternity Services NHS England Women’s Specialised Services Clinical Reference Group representative for the North of England