Some really exciting developments with #MatExp Whose Shoes? at the moment.
Bromley MSLC produced a ‘one year on’ report following up on their Whose Shoes? workshop at King’s College hospital using “I said, I did” as a framework to list all the fantastic outcomes that had come from pledges made on the day.
Language continues to be a big issue for women and families, but some great initiatives are now happening. Building on the Whose Shoes? workshops, Leeds and Colchester in particular are working on specific language challenges. I came up with a ‘Negativity Bingo’ and had great fun with my team at the NHS Fab Change Day #DoAthOn event launching #DumptheDaftWords.
I have been getting some exciting invitations to speak about building social movements and of course gave #MatExp a big shout out in my talk at the launch of #AHPsIntoAction, they have invited me back for a longer keynote session at their annual conference in June.
More hospitals are coming on board with the Whose Shoes? approach – the energy is particularly strong in London, the West Midlands and the South West regions. It has been great to present on several occasions now with Catherine MacLennan and Emma Jane Sasaru and to see people learning so much from their courageous sharing of their lived experience.
This slideshow requires JavaScript.
Last Friday, 3 Feb 2017, we were invited to present a #MatExp Whose Shoes? session to get some good discussions going as part of a packed event launching #PanStaffsMTP in Stafford. We concentrated specifically on continuity and perinatal mental health. This is the county-wide transformation programme to improve maternity experience in Staffordshire to implement the national ‘Better Births’ vision. This informal film gives you a flavour.
We are proud of the crowdsourced ‘Nobody’s Patient’ project and thank everyone for your fantastic contributions. We now have over 120 new Whose Shoes? scenarios and poems and the new resources will be made available shortly to all the hospitals who were existing customers. Florence Wilcock, Sam Frewin and I are finalising the supporting toolkit and collating the case studies, ahead of our ‘wrap up’ event in March. We are trying to pull together lots of ideas for positive change, with or without a workshop. I hope you are enjoying the regular Steller stories, including Florence’s monthly reports.
Wonderful to see everyone doing such amazing work, speaking all over the place, building networks, spreading the word and generally making great things happen.
This post has been written for the #MatExp campaign by Claire Flower, Clinical Specialist Music Therapist and Joint Team Lead for the Chelsea and Westminster Hospital NHS Foundation Trust. Our thanks to Claire and her team for their support for #MatExp.
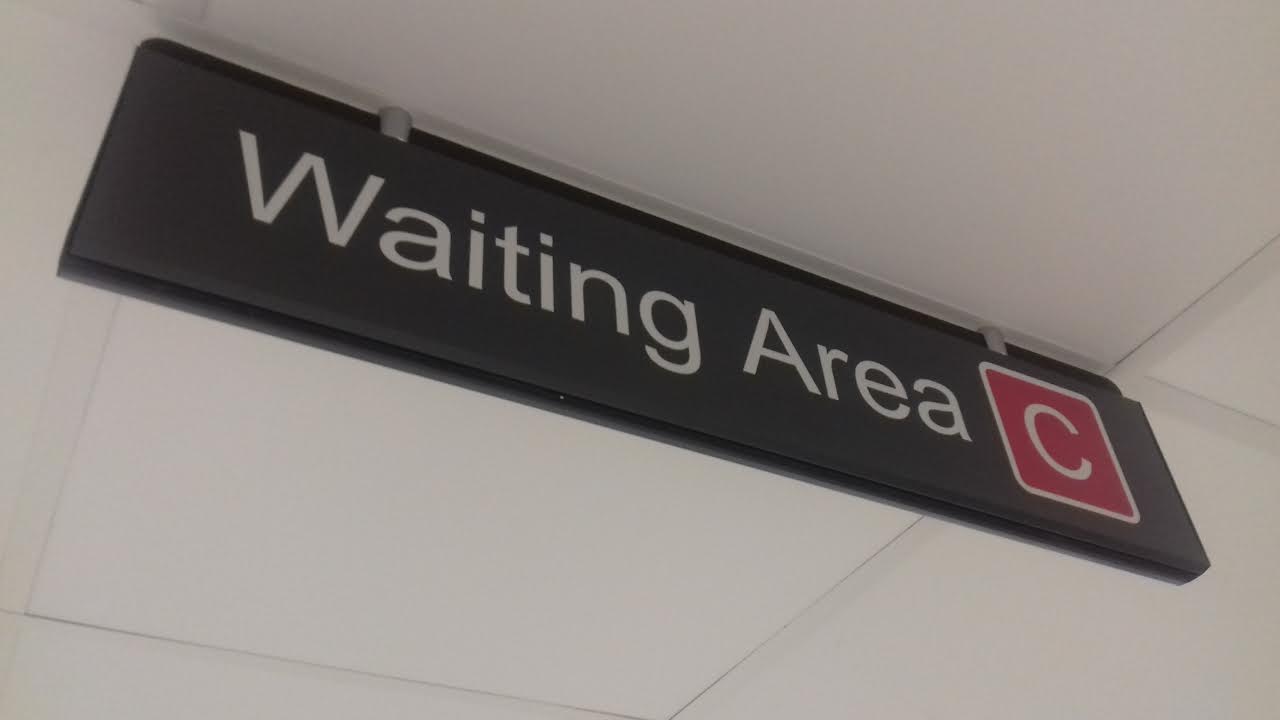
‘Music While You Wait’ is the working title of a project we’re recently been running in maternity care at Chelsea and Westminster Hospital, London.
My name is Claire Flower, and I jointly lead the music therapy service here at Chelsea and Westminster hospital. We have had a large children’s music therapy service for many years in the Trust, but recently we’ve had specific funding to explore how music is used by, and can be helpful for, women through pregnancy and birth. The project title – ‘Music While you Wait’ – has seemed fitting, both because of pregnancy itself being a waiting game, but also because the project has been based in the antenatal waiting areas of the hospital.
In conversations with midwives, doctors, pregnant women and partners one of the themes which kept popping up was that the experience of attending, or working in, an antenatal clinic can sometimes be extremely stressful. People told me that at busy times the clinics are often full and noisy, some women may have children with them which brings its own pressures, some may have lengthy waits to be seen, and some may be anxious about being there for all kinds of reasons. As one woman said to me, ‘not everyone here is happy’.
There was a real, shared interest in exploring together how music might be one way of making the experience of the clinic better for everyone, lowering stress levels, reducing anxiety, and giving different opportunities for social contact and connection.
We agreed that I would attend 6 different clinics, offering live music, as well as talking with women, partners and staff about music in pregnancy and beyond. And so we started – wheeling an electric piano into the waiting area, playing a range of music, talking, and being prepared to see what unfolded.
Over the weeks, I kept a journal, describing events in each clinic, and thinking about them in preparing for the next one. Looking back at them now, they give a flavour of some of the moments which characterised the project.
For example, how the piano music was received by women coming to the clinic…..
‘One couple arrive, and as they walk in she looks across and says quite loudly across the room, ‘oh it’s you!’. There’s surprise from both of them that the music is live, they’d assumed it was the radio. ‘There’s just something about having the person, you know?’ she said.
On the same morning….
‘Another woman smiles frequently at me as I play and she waits. In fact, she moves from sitting with her back to the piano, to facing me and sitting closer. As I stop to respond to someone’s comment, she agrees that it’s lovely, and says she was just texting her sister to say how lovely it is to sit and listen to. Makes me think that music is doing its work of rippling outwards to unexpected places!’
In this busy clinic, women often come with children – quite a challenge if there’s a lengthy wait. When one woman arrives with two energetic young children, looking quite exhausted, I wonder how I might be able to help with some music for them….
‘I come away from the piano, and bring out some small instruments for us to use, crouching down with them to sing. Mum joins in, and the children begin to sing and dance, moving rhythmically to the music. Looking around, I see other women smiling at the children, or even moving a little to the music…. After a good play, we agree to put the instruments away (I’m really not sure how the sound levels will have been for the poor midwife in the room nearest to our impromptu band!), and somebody in the room suggests it’s ‘time for a lullaby’, I return to the piano, and we have a gentle rendition of Twinkle Twinkle, one of the children ‘twinkling’ at the top of the keyboard.’
And then there was the morning when this happened…..
‘As I’m playing, one woman, quite heavily pregnant, walks in, looks towards me smiling, and walks towards me. She approaches so confidently, and with such a smile that I wonder whether we know each other, or that I’ve forgotten meeting her here previously…..’
What unfolded from that point was one of the highlights of the project for me, but she’s best placed to tell you about it herself….
“I am a professional violinist. In July 2016 I was almost 9 months pregnant with my second child and was suffering from gestational diabetes. So every Tuesday until my C section I had to go to C&W and be assessed by a diabetes specialist nurse or consultant. I was very anxious and tired beyond belief. On top of that, more often than not there was a rather long wait for the appointment.
Needless to say I wasn’t looking forward to Tuesday…until one day when I walked in and heard music. There was soft classical music coming from a speaker or two (I thought for a few seconds until I spotted the real source, at the back of the room). SOMEONE (not something!) was playing that lovely music. How amazing, and how very rare…
I walked straight towards her with no doubt in mind of what I was going to do. I had to come here, bring my violin and play with her, even if it was just for a few minutes! I had been pregnant and breastfeeding for three years by then and playing the violin had LOST ITS place in my life. I did miss it desperately and said it. To my absolute joy Claire invited me to bring some music as well the following Tuesday, before my appointment and play with her for almost an hour. We discussed the music in detail (not everything suits so I took her advice and offered to also bring something a little different to see if and how it might work).
I counted the days until my next appointment, even managed to practice a little for the first time in years, searched for my beloved but long forgotten music and didn’t think of anything else other than how wonderful it will be to join Claire and play for everyone there who was going through the same hard times as I was. It was also the first time my daughter listened to me play the violin in public. I felt like the luckiest and most privileged woman on earth (no exaggeration here!).”
For everyone who was lucky enough to be working, or coming to the clinic on the day when this happened, it was a magical moment. It certainly ticked the box of seeing how music might make the antenatal clinic experience better for everyone there.
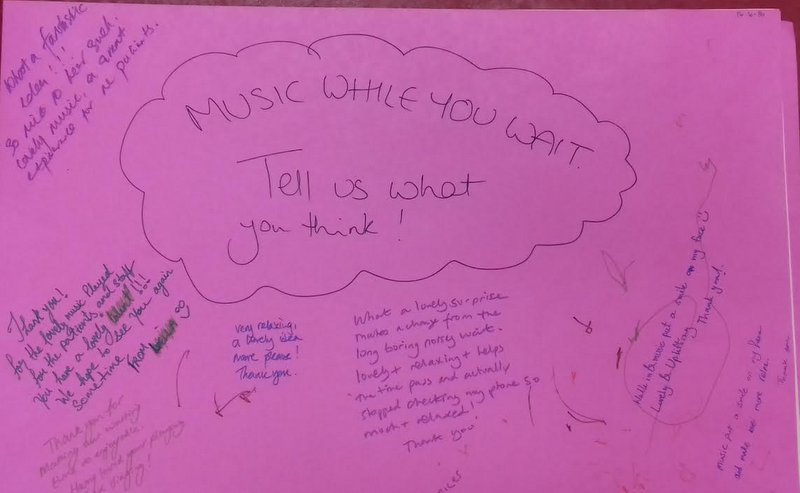
We’re writing the project up now, using, among other things, the comments which were written and drawn for us by women, children, staff, and partners in each session.
And we’re discussing what we do with it next, which might mean developing it further in the waiting areas, as well as thinking about how it might translate to the wards.
As Viki Girton, Lead Midwife for Antenatal Clinics says ‘Music While You Wait helped to create a relaxing environment for staff and patients… having more would be fabulous to improve maternity experiences and patient satisfaction here’.
I love being a music therapist, but being able to step into the maternity world and work with such a great group of women, staff and families has been a new pleasure. We’re really excited to have conversations with anyone interested in where we take this next, and how music therapy might play a part in #MatExp!
When you think of a competition, what do you typically think of?
An application form with lots of dull questions ✅
A raffle ticket with a lucky number. Not necessarily yours. ✅
A dodgy message flashing on your phone saying you have won £1 million. Claim your prize NOW!!
Well, as many of you will know, ‘#MatExp Whose Shoes? ‘is a bit alternative. So we are giving you endless alternatives as to how you would like to enter the competition. We are not big fans of labels, boxes and standardised formats So just take a look at the link below to see the areas we would like you to think about and then let your creativity loose as a goose and see what you and your people come up with!
And if you don’t know what ‘#MatExp Whose Shoes?’ is about, where have you been for the last two years? 😉 Loads of material here on matexp.org.uk or by browsing the web. And one of these days Gill Phillips, creator of ‘Whose Shoes’ will get round to updating her website – but she has just been far too busy tweeting and building momentum on Twitter @WhoseShoes.
Please also help spread the word. We are hoping that lots of people who are not familiar with social media will get involved and will get drawn in by the MatExp magic and find that it is fun to link with others who share their passion, way beyond the confines of their department, hospital or local area.
Click the link below to download a PDF file which contains further information and an entry form. Good luck!
With the launch this week of #YourMaternityCare campaign by the Care Quality Commission (CQC) encouraging women to share their maternity experiences now seems as good a time as any to share some of my thinking and importantly ask some questions.
To be clear I am not going to talk scientific methodology, survey design or validity, I am simply going to share some personal ideas as an obstetrician and a member of the #MatExp gang and question if we could use the survey to challenge ourselves in a more creative way.
What sort of impact does this sort of survey have on the care women receive?
The answer to this may depend on how you view the results. It can be examined at a national level looking at care across the country and comparing with previous years to look at trends and themes.
Undoubtedly this survey showed better experiences overall than in previous years and this is good news. An excellent example is the increase in the number of women receiving care before 10 weeks of pregnancy, with a big potential impact on eventual outcome. It is important to take time to give ourselves a collective pat on the back and celebrate those improvements as it can be so easy to focus only on the negatives.
For a great visual overview, take a look at the infographic produced by Picker.
On a regional level the 2013 Maternity survey and the negative results of some London Trusts was actually one of the sparks that led to the London Maternity Strategic Clinical network focusing on ‘Patient experience’. Therefore it directly led to the ‘birth’ of #MatExp and our collaboration with Gill Phillips to produce a maternity version of her Whose Shoes game and development of a workshop toolkit & examples of best practice.
So that’s another positive: the resulting #MatExp change platform and community of people interested in improving maternity experience therefore could be said to be a direct result of the 2013 survey.
We can examine hospital level data and see how a maternity service changes over time, and how women respond on specific questions. This can help us identify a particular area that needs improvement, such as continuity or postnatal care, as well as giving positive feedback about what is working well. It can help us benchmark our services against others locally or nationally. It is undoubtedly a valuable data point even if it has limitations and exclusions however it is only one of many ways we should be looking at feedback.
Most Trusts will have an effective governance system meaning that the results will be reviewed and circulated, an action plan devised and those actions systematically ticked off when completed.
We need to be cautious as it can become all about process and tick boxes if we are not careful, held at management level and a little detached from both those in daily practice and our service users.
I wonder how many Trusts have worked proactively with their Maternity Service Liaison Committee (MSLC), staff and service users since they received their individual 2015 reports to identify what improvements would have the biggest impact for their women and to look at how their survey results correlate with other methods of feedback they use?
Moving on to some specifics now, the very first sentence in the recently published CQC response to the survey results is a shock ‘There are almost 700,000 live births each year in England. Having a baby is the most common reason for a hospital admission.’
Why is this?
According to the National Tariff benchmark data 65% of women are ‘standard’ i.e. do not have a complicated antenatal period and therefore are ‘healthy’ pregnant women.
Therefore, the first challenge from the results is why are so many of these births happening in hospital. It probably has something to do with the fact that the survey showed 63% of women who have given birth previously were definitely given enough information about where to have their baby, falling to 53% of women giving birth for the first time. This presumably means large numbers of women are not getting adequate information.
I’m not going to recap NICE Intrapartum care 190, but we know it provides evidence that for healthy pregnant women who have had a baby before we should be explaining birth at home or in a midwifery led unit is likely to have less intervention and the same outcome as delivery in a hospital.
Across the survey results first time mothers seem to be getting a worse experience with consistently lower results than women who have given birth previously. Is this because we are doing something different for first time mothers, is this because we should be doing something different or is it simply that the different groups of women have different expectations? Do first time mothers have higher expectations and are then disappointed whereas mothers who have given birth previously have lower expectations as they know what it was like last time?
In amongst some good improvement scores remain worrying minorities. 89% of women said that during their antenatal care they were “always” spoken to in a way they could understand – up by 7 percentage points since 2007 (82%). However, this means that 11% were not “always” spoken in this way. 87% of women reported that they were always treated with dignity and respect during labour and birth compared to 85% in 2013, but what about the 13% that were not? Surely these are the fundamental basics of care and should be true for every single woman. What are we doing about these women? Can we identify who they are, are there specific groups we are not catering for or not understanding what they need?
Don’t even get me started on lithotomy: ‘The proportion of women being in a position of lying with legs in stirrups whilst having a normal vaginal delivery has seen a steady increase over the past few years going from 17% in 2010, to 19% in 2013 and 22% in 2015’. What on earth is this all about? In 2015 I undertook a lithotomy challenge on NHS Change day and you can read about my experience in the blog I subsequently wrote.
Postnatal experience is clearly lagging behind antenatal and labour care with much lower figures sitting in the approx. 50% region on all aspects of care including physical and emotional wellbeing. Collectively we need urgent action to address this? But the need for collective action raises a problem. Within the NHS we now have this terrible dilemma collaboration versus competition.
The CQC Response to the survey results clearly highlights Trust who have performed better or worse than expected in the last two surveys. If we accept that these results are valid and not a difference in expectations or different for other reasons, then as a simple solution we could potentially buddy up good performing Trusts with poor performers.
However, Trusts are individual organisations. The strategic clinical networks and NHS England can influence, but there is no obligation for Trusts to help others. If we work at a good Trust what is the incentive to share what works? Pure altruism goes some way, but when you face difficult budget choices and competing demands collaboration can be an easy casualty, and as health care professionals what responsibility do we have to try and improve quality outside our own immediate practice?
I certainly don’t have all the answers. For me #MatExp is some attempt at trying to improve and discuss many of these issues on a broader scale, ignite a lively conversation about maternity care and to encourage others to think that they can influence positive change however big or small.
Florence Wilcock
2016
If you are interested in joining the conversation or taking action on improving maternity experience in anyway jump in and join us on Twitter (find tweets tagged #MatExp), join our group on Facebook, or send us a message.
I was asked to do a talk to student midwives at Salford University this month on the topic of “Women’s Voices” in maternity care. As part of my presentation I included the voices of the midwives who work in maternity care, and a reminder that there are many other women for whom maternity care is their professional, as well as perhaps their personal, experience. “Women’s Voices” in maternity care should cover the midwives, obstetricians, health visitors, doulas who care for us, as well as the women giving birth.
So I decided to start a series of blog posts on “Women’s Voices in #MatExp” from the point of view of those working in maternity, and this is the second of those. This is Maddie McMahon’s experience of being a doula. Thank you so much to Maddie for agreeing to write for us.
You can read the first blog in the series here. And yes, I will be doing a “Men’s Voices in #MatExp” series too. Because this campaign is about all voices.
Helen.x
*********************
Maddie McMahon is a doula, doula mentor, doula course leader and breastfeeding counsellor in Cambridge. She is also a member of the board of Doula UK. She supports women using the same hospital she, herself, gave birth in and has been a staunch supporter of that hospital ever since, sitting on the MSLC since 2004.
She is author of ‘Why Doulas Matter’, published by Pinter & Martin in 2015.
I have been a doula for 13 years and have supported hundreds of women, either before their birthing, during their labours or afterwards. I have been facilitating an initial doula preparation course since 2008 and have been mentoring doulas and intimately involved in the evolution of the doula community in Britain since early on in the history of Doula UK.
In all those years I have learned more about what a doula is not, than what a doula is. Every time I think I might have got a handle on the ‘definition of a doula’, my understanding and perception shifts again. The definitions that do the rounds on the internet can be shallow, to say the least and, at best, undermining and dismissive of the incredible talents and abilities that women bring to this role.
I see all sorts of women being called to serve the mothers of their communities. There are women, like me, who felt a gaping hole or a contrast in how the time of transition into motherhood can feel so very different with and without psycho-social support.
There are women who feel betrayed and let down by their health professionals. They may be fighting birth trauma or PTSD or just a deep sadness.
But there are also mothers joining the community now who have been supported by a doula themselves, feel ecstatic about their birth experience and have been inspired to pay it forward.
There are women who, despite all their protestations of loyalty to their careers, found that motherhood remade them, in a fundamental way, bringing them to a realisation that ‘work’ needs to fit around children, nurture our souls and service our communities if it is to be truly worthwhile.
Some come to the role from an academic direction. They are incredibly bright PhD students or researchers, for example. They are interested in motherhood from a sociological, anthropological, political, psychological or philosophical standpoint. They may be activists or campaigners.
Then there are the Human Rights doulas, the ones interested in things like consent, maternal rights and responsibilities. They may have worked in sex and relationship education, or in women’s advocacy or legal settings.
Related, are the doulas who come to the work through their work with social services, or other support of vulnerable or hard-to-reach groups. I know many doulas who started off working with Birth Companions, working with women in prison, or as Homestart volunteers, in teenage pregnancy units, or are Maternity Support Workers..
And there are those who see birth as merely one step on a female journey, all of which deserve emotional and practical support. They support their community of women through menarche, marriage and divorce, abortion and baby loss, birth, breastfeeding and beyond, right up to menopause and sometimes doula families through the last and ultimate transition – death.. They are the white witches, the humanists and the pagans, the searchers for and creators of ritual and ceremony, the red tent facilitators, the women’s circle founders…
The ‘breastfeeding doulas’, through their voluntary work as breastfeeding counsellors, come to see that the challenges women face initiating and maintaining breastfeeding are often down to wider social and familial pressures. They begin to see these pressures and understand that, much as we can suggest to women to go home, sit and enjoy nursing their newborn, it doesn’t magically get the washing up done. The hour they can spend with women in the breastfeeding clinic doesn’t give them the space and time to explore the social attitudes that invisibly pressurise them to supplement with formula, or sleep train, or help their partner take a more active interest in the baby.
Related are the ‘babywearing doulas’ and the nanny and childminder doulas who, again, have come to the work through close contact with new mothers…who have seen close up that mothers of newborns need a particular type of peer support that the doula ethos perfectly encompasses – that time, and space we can give. That unconditional listening ear. That ability to help a mother access and trust her own mothering instincts. The way a doula supports a mother to do the mothering, and supports the partner/father too to step up and find his skills and abilities as a parent. The doula way of somehow ‘de-medicalising’ motherhood.
And lastly, but certainly not least there are the midwives. Some are retiring. Some have been out of the midwifery loop for a while and are choosing between a return to practice course or the doula route. Others are, quite literally and very sadly, at the end of their tether with the NHS and the constraints it places on midwives and mothers. They often feel like they can’t practice in the way they would so love to; supporting women through the whole journey. Continuity of care, pressure to follow guidelines and management that pays mere lip service to issues like individualised care, consent and compassionate care, have driven them to throw in the towel.
As you can see, many of these women might be bringing baggage to the role. They may well have conscious or unconscious axes to to grind. It is through doing a doula course that we aim to create a safe space to process and contain this baggage, to become conscious of our worldview and how it might create the version we see of the world. We begin to practice ways to bring ourselves back to the women and families we serve, to see the world through their eyes and to therefore support them unconditionally and without judgement. Because it is this lack of an agenda, a lack of micro-managing guidelines and regulations that allow families to relax into our presence and for doulas to become a trusted part of the family.
All experienced doulas know that we are, in some respects, extremely lucky. We revel in the luxury of not having to follow guidelines, merely supported by the philosophy and Code of Conduct that our community has created for itself. We are free to build deep and abiding relationships with women, their partners and their children. We get to listen to her deepest fears and anxieties, support her to find solutions to her practical challenges and gain a deep understanding of her desires for this birth and beyond. We never, ever make the mistake of assuming that women might hold the experience of childbirth above the safety of themselves and their babies. Every working day teaches us that this idea is ludicrous. We see the birth trauma, the family dynamics, the physical and mental challenges that explain a woman’s choices. Really, really close up, it all, always, makes sense.
So, we have this deep, vital knowledge of a woman and why she wants what she wants. We have seen her do her research, read studies, talk to professionals, lay/peer supporters, friends and family. She has worked it through in her mind and her heart. She understands the risks and benefits of the choices she is making. We walk with her on this journey, every step of the way. So, when that journey gets to the point where we might be sharing a space with midwives or obstetricians, we have to seamlessly move from being a team of 2 or 3 and move aside in a loving way to bring these professionals into the circle so that we can create a loving circle around the woman.
That dance can go in a number of different directions, depending on the circumstances. There are some common challenges that can prevent good relations between doulas and staff in the birth room. One of them is possessiveness on the part of the doula. It’s wrong, and egotistical and something that shrivels as she gets more experienced, but I do think we can be forgiven, just a little bit, for thinking that we know better than the maternity staff what the woman wants and needs. It can make us a little defensive when they appear not to have read her birth wishes. It can make us a little grumpy when someone comes into an atmosphere that we have set up according to her wishes and switch on the lights and start talking loudly.
Perhaps we aren’t always super-skilled at handling those kinds of interactions. And perhaps there is more going in underneath those interactions than we doulas are sometimes aware of. If I ask if it’s possible for us to find a floor mat for a labouring woman, and that midwife has just been having a conversation with a colleague about doulas and how we have a ‘natural birth and all costs’ agenda, she may read more into my request than I intended.
If a VBAC couple ask a doula to tell the midwife they don’t want continuous monitoring, how can that be handled? The midwife may not know that they have done their research antenatally and made an informed decision. She may wonder who the hell this doula is, who appears to be talking for the couple. How does a midwife know that these parents aren’t being coerced or persuaded into a course of action without understanding all the possible ramifications? How does that midwife know she will be supported by her colleagues to support this ‘off-piste’ decision?
Sometimes we are aware that there is an underlying atmosphere in the room based on these myths and misunderstandings about a doula’s role. Most of us have realised that it’s common for midwives to think that all doulas are frustrated, wanna-be midwives. Some think we meet the clients for the first time when they are in labour. Many think we are making an inordinate amount of money. Some see the intimate connection we have with the couple and are forced to contemplate why they, themselves were drawn to birthwork in the first place and how it hasn’t quite turned out the way they longed for.
Other times, when a member of the obstetric staff is in the room, the presence of a doula can wrong-foot and confuddle them no end. They are talking to a couple, counselling them through their options, and they suddenly turn to the anonymous, unnoticed woman in the corner, and ask her what she thinks. Even more confusingly, sometimes she asks a question that sounds surprisingly knowledgeable, or asks the couple if they need anymore information about the risks and benefits, or wonders whether there is an option to do nothing at all. She may suggest a few minutes of alone time to think and usher everyone out of the room. The woman they assumed to be Auntie Doris, is suddenly orchestrating the situation somewhat. Unsettling to say the least. Worrying, perhaps, and possibly anger-inducing.
After the baby is born and a community midwife or Health Visitor visits, it can be hard for her, in the time allowed for the visit, to get a real handle on who this woman is who appears to know her way around the kitchen and hangs around in the same room for the duration of the visit. Can the mother talk freely in front of her? Is the doula giving out of date or wrong baby care or breastfeeding advice? These concerns remain unsaid, but can prevent a real human connection.
We know that sometimes, both doulas and staff bring baggage, myths and ignorance of each other’s roles into the birth room. And most of the time, it is our communication skills, or lack on them, that prevent a deeper affinity and closer working practices developing.
All those talented women, with enormous hearts and the energy to support birth, whether they are clinical or lay, deserve to have the love and support of each other. We all have a massive amount to give.
Doulas are responsible for some of the most positive support networks in recent times: The Positive Birth Movement (PBM), Birthrights, the VBAC and Birth Choices support groups, social media support, breastfeeding support to name but a few. When those support networks work most beautifully is when lay women and midwives work together as equals, loving and respecting the complementary threads we each bring to the work. By working alongside each other, we both learn and grow, for the benefit of the mothers we support.
These communities we build, the rituals we rebirth – these are the special and truly valuable aspects of the doula movement. Perhaps now is the time to validate this grassroots work and build on the models we have set up, that are clearly spectacularly successful! 170 PBM groups in the UK alone. 40,000 followers of Dispelling Breastfeeding Myths on Facebook, 10,000 followers of Birthrights. Community support and advocacy is clearly needed – in fact women are hungry for it. And a lot of this community-building work is about supporting health professionals too. Many doulas work to provide community support to their local student midwives, or welcome community midwives to their mother-support groups. We raise money for our local hospitals, sit on MSLCs, try to raise awareness of the challenges facing maternity services, even march alongside them, with placards raised.
We like to think of the mother, at the centre, as the sun, with her supporters orbiting around her in elliptical trajectories. Sometimes the midwife moves in closer, sometimes the doula or the doctor. We move further away to make space, to allow the mother room to make decisions and find her own answers. We move in closer when she needs physical or emotional support. We recognise each other’s skills and talents and make way for each gift to be bestowed with love and appropriacy.
When we all work more closely together, we see for ourselves how much the doula philosophy of information without agenda, unconditional emotional support and listening without giving advice have a tangible effect on outcomes – not just in birth statistics but on the mother’s state of mind and her emotional and physical ability to mother her infant.
Many doulas know that some of us could learn a little more humbleness from midwives and Obs and understand a little more quite how challenging, heart-breaking and downright soul destroying their work can be sometimes. And perhaps they could learn a little from us – about compassionate listening and keeping care woman-centred, tailored to her personality, preferences and anxieties. They could learn how our depth of relationship with a family may give us insights they don’t have, and not to feel defensive about that, or jealous.
So how can be build better understanding and cooperative working practices?
We see a lot of wonderful stuff going on already: doulas being asked to meet and speak with student midwives, so that they learn about our role from the beginning. It would be good if this were extended to student doctors too.
Some doula preparation courses will allow midwives and student midwives to sit in, for free – to get a taste of the doula community and an in-depth understanding of the many variations of the doula role.
Many doulas sit on MSLCs and Labour Ward Forums, which is a great way for us to share stories and client experiences and to learn more about the workings of the service and the challenges it faces. Mutual empathy is often very effectively built this way. It can work even better when the staff come out to sit in our forums – to visit our pregnancy support, breastfeeding and parenting support groups.
Social media is one way forward. The relationships and mutual respect between doulas and midwives has blossomed since we have begun to get to know each other on Facebook and twitter. We can really help each other – doulas helping the campaign to spread the knowledge of Optimal Cord Clamping springs to mind, or spreading understanding and therefore driving consumer demand for the ‘gentle’ or ‘woman-centred’ caesarean and ‘seeding the microbiome’. We are also able to provide each other with emotional support online and these friendships sometimes benefit mothers in very tangible, ‘I know exactly the right person for you to talk to’ kind of way.
We’d like to see us working together to create more models that provide psycho-social support for more vulnerable and hard-to-reach groups. That 14 year old girl may well have a wonderful specialist midwife to support her, and perhaps the young parents group at the local children’s centre to tap into. But wouldn’t it be wonderful to find out whether any of the local doulas have experience in this area or were young mothers themselves? Sometimes someone coming along who isn’t wearing a badge or a uniform, can make all the difference.
What about those women who ask for elective c-sections with no clinical indication? How many units have specialist counselling services for tokophobia or birth trauma? How many doctors or midwives suggest to women that a bit of peer support might help? Signposting to ‘patient support groups’ can make all the difference, as many women’s accounts of the effect of other mother’s positive stories attest.
There are doulas who have experience of working with women in prison, doulas who are also clinical psychologists, doulas who work exclusively with young mothers, or who work closely with Social Services or Homestart. There are doulas who have a lot of experience building rapport and trust with women who are suffering huge anxiety, and doulas who work with women with particular conditions, like Hyperemesis. There are doulas who specialise in breastfeeding support and who are also Breastfeeding Counsellors or IBCLCs.
Some of us receive direct referrals from maternity staff. Some don’t. Some hospitals have built formal, cooperative models that incorporate doulas, in a voluntary or paid capacity, into the system in some way. Sharing best practice, spreading ideas, building on the successes and working sustainability, mutual knowledge sharing and auditing into the processes seems to us to be the way forward.
Given that doula support appears to have a growing body of evidence to suggest we can increase normal birth rates, minimise cesarean sections and save the NHS money, it is surely time to begin to formalise our partnerships.
So if you are a health professional, why not resolve to find out about the doulas in your area? Perhaps invite them for a cup of tea – they’ll bring the cake.
I was asked to do a talk to student midwives at Salford University last week on the topic of “Women’s Voices” in maternity care. As part of my presentation I included the voices of the midwives who work in maternity care, and a reminder that there are many other women for whom maternity care is their professional, as well as perhaps their personal, experience. “Women’s Voices” in maternity care should cover the midwives, obstetricians, health visitors, doulas who care for us, as well as the women giving birth.
So I decided to start a series of blog posts on “Women’s Voices in #MatExp” from the point of view of those working in maternity, and this is the first of those. This is Dawn Stone’s experience of being a midwife in the NHS. Thank you so much to Dawn for agreeing to write for us.
And yes, I will be doing a “Men’s Voices in #MatExp” series too. Because this campaign is about all voices.
Helen.x
*********************
Dawn Stone is a 27 year old midwife living and working in central London. Dawn qualified as a midwife in 2014, and is passionate about improving experiences for students, midwives and women.
It’s an insignificant Monday afternoon in SE London to many. It’s beautifully warm, people are rejoicing in beer gardens as they finish work, I hear the giggles and shrieks of laughter from a nearby park as I walk home. It’s an idyllic summers day; and yet somehow it feels cold to me.
I’m on my way to see my GP. I made the appointment last week, but it feels fortuitous to have this lifeline today. Because today, of all the 303 days I’ve been a midwife, it feels way too much to bear. And I need some help.
I’ve been here before. A few months ago the feelings on inadequacy, frustration and disappointment reared their ugly heads and I made the same journey to my GP, begging for help. She, to her credit, was wonderful but the medication she prescribed was not. I went back to work but felt like I was going through the motions. My appetite was reduced, I hadn’t slept a whole night in months, and I constantly had a knot of tension in my stomach whenever I thought about work.
What do I do? I’m a midwife. And it nearly knocked me off my feet completely.
I trained as a midwife in a busy central London hospital, which often felt like a baptism of fire and was definitely not what I was expecting. I was lucky to witness amazing births, incredible women, and unfortunately, at times, disappointing midwives. It seemed as though some had lost the ability to care about the women as well as for them; and so I qualified with a goal. Be the best midwife I can be, and never forget the power and importance of being kind. It sounds so simple when you write it down!
Upon qualifying, I moved to another busy central London hospital, and began working as a bona fide midwife, alongside a group of also newly qualified midwives who would become my lifeline. Together we jumped into this chaotic and intense career, and discovered that being a student midwife does NOT prepare you for being a midwife. Not at all. You have no idea as a student the enormity of every decision you make – that lochia is normal, that baby is not jaundiced, that baby is unwell and needs an urgent review. And on and on it goes; a hundred different decisions, all before lunchtime and all before you’ve had a drink or something to eat. And if you’re lucky, you’re figuring this all out in an environment which is supportive and conducive to learning, where you know you have more experienced midwives to lean on and ask ‘Does it get better?’
If you’re unlucky, you’re essentially told to suck it up and keep going. Never mind that you’re awake at 4am going over and over the shift from yesterday, thinking about each woman and baby, and what you handed over – did you forget something? You definitely did. Shut up mind, go to sleep. Except you definitely did forget something because you did a blood sugar on the baby in bed 9 before you left and you forgot to write it down. It was normal, thankfully, but should I ring? No. It’s 4am and it’s your day off. Go back to sleep.
Working on a busy 50 bed AN/PN ward can feel like being on a carousel that’s spinning and spinning; there is no slowing down, only jumping on, and trying to stay upright and facing the right way.
When I arrive for my night shift, I look at my workload and I hope for an okay night. I have a mixture of 2 high risk AN women (for close monitoring of their severe PET), an IOL for post dates and 4 PN mums & babies – all of them are on obs overnight, 1 mum is also on IVABX for sepsis, and my colleague has just handed over that one of the babies hasn’t fed for 6 hours. I take a deep breath, try to quell the tide of worry that’s swirling in my stomach, and do the only thing I can do. I make a plan. I read the notes, I look at the blood results, and I try to prioritise what needs doing and when. I say hello to all 7 women, some of whom I know, and I begin to do what needs to be done.
And I’m sorry if I couldn’t sit with you longer during your breastfeed. I can see your baby is feeding well but as a first time Mum you need some support and guidance as you learn this new skill. I want to sit with you, and gently reassure and reaffirm you as you confidently latch your baby to your breast. But I can’t. Because I have 6 other women, and 3 other babies who need me. So I do what I can, and then ask a maternity support worker to step in, and do what I cannot.
I’m sorry my checking on you and baby felt like a list of questions, one after the other, relentlessly. I know this isn’t the best way to elicit how you feel about this huge shift to parenthood, and I may not ask the question you need me to, and so your niggling worries remain unchecked.
I’m sorry I have to wake you at 2am, and 6am, to check your blood pressure. The medication you’re on to manage it is very good but we need to ensure its effective, and the middle of the night BP is actually one of the most useful. I hate waking people up, and I know you don’t mean to swear at me as you grumble and sigh, before brandishing me your arm, but it still hurts to hear. Thankfully your blood pressure is normal, and I can tiptoe out & leave you to rest.
As I walk past the desk, I see my bottle of water, next to my colleagues. All untouched.
I’m sorry you’re in a mixed bay of women, and you can hear babies crying as your labour is starting, and it’s not dark or quiet as you need it to be. I’m sorry you’re quietly sobbing on the edge of the bed as you try to get through this contraction without making too much noise and waking the sleeping bay. I’m sorry I can’t be with you, talking you through your contractions and helping you to relax and reduce the fear/tension/pain cycle. I know that you need me, but I have obs to do on 2 of the babies in this bay, and I need to check on one of women with raised BP as she’s on the monitor and I hope it’s ok as I had to dash out of the room once it was on. I’m sorry I’m only half with you as I rub your back, as I’m juggling my outstanding jobs in my head. Thankfully, some codeine and a warm baths eases some of your pain, and you spend a few hours soaking in there, feeling much more relaxed.
I’m so relieved.
I’m so relieved that your labour didn’t progress rapidly, and your baby wasn’t born on the ward.
I’m so relieved all of your babies obs were normal, and they didn’t show signs of an infection.
I’m so relieved that the heavy bleeding you complained of turned out to be normal blood loss, and you’re not having a haemorrhage.
I’m so relieved your blood pressure was normal, and you’re not feeling any symptoms of pre eclampsia.
I’m so relieved when you come to me at 4am, as I sit at the desk gratefully drinking a coffee as I relish the middle of the night peace that’s descended, and tell me you latched your baby on yourself & it felt like a good feed.
I’m so relieved. I’m also hungry, and tired, and the water has remained untouched although I have slurped a coffee my colleague made for me.
This shift has been busy, and stressful, and required me to constantly assess, juggle and prioritise. But it’s not extraordinary. It’s a typical shift in a typical London hospital on any given day. The women are grateful, and I leave with a small sense of doing a good job.
Until I return the following night to be told I didn’t do a VTE risk assessment. And the dyad I helped with breastfeeding are now mixed feeding as she felt her baby wasn’t getting enough. And the mum who labour began during the night is still on the ward, awaiting a doctors review to formulate an ongoing plan. And we’re short staffed. And I can feel a headache coming on as I didn’t sleep well, worrying and replaying the previous shift over and over.
With such unrelenting pressure, is it any wonder I’m crying to my GP, telling her how unhappy I am, how tired, how morose? And is it any wonder she doesn’t bat an eyelid when I ask for antidepressants, and a sick note?
*********************
#MatExp is a campaign about ACTION! So what can be done? We have already written about how it is Time to Act for Midwives, but as this recent post on Sheena Byrom’s blog demonstrates, these issues are not isolated and they are not yet being taken seriously.
Sheena kindly commented on what Dawn had to say:
“Dawn’s reflection of her experience trying to do her work as a midwife is distressing, and tragically, Dawn is by no means alone. I receive regular emails from midwives and student midwives who feel desperate, unable to go on, and ready to leave our profession.
I sincerely hope the National Maternity Review report will kick start the much needed radical reform of maternity services. If we can’t support, care for and nurture maternity workers to provide safe, effective high quality maternity care, we have an unsustainable situation.”
Community Outreach Midwife Wendy Warrington also commented on Dawn’s experiences:
“This could have been written by me and the majority of my midwifery colleagues as accurate, and to be honest been there themselves me included! I came back to work after nearly 3 weeks off and Monday morning I had a knot in my stomach when I turned on my work phone and strolled into the community office. Fortunately all was well, but that was due to in the run up to Christmas ny starting early working at home, finishing late and putting written plans in place. Four women on my caseload delivered and I have high risk caseload due to safeguarding concerns.
In terms of improving the situation there needs to be a shift from the blame and bullying culture that seems to be prevalent within the midwifery profession and the NHS as a whole. Senior management with their expectations bully staff below them and this continues down the pecking order. Midwifery sadly is still very hierarchical. Also the public perception and expectation has shifted from when I first started. There does not seem to be the respect from the public as in days gone by . The “where there’s a blame there’s a claim” culture. Cuts to funding, staff shortages and the media have not helped.
Sadly I am counting down the days until retirement as are many of my colleagues.
So how to improve the situation? As colleagues we should nurture and support one another, and small pockets of us do. I personally have found my escape using Twitter and Facebook groups. Realising there were others out there who felt and thought like me and had not had the passion snuffed out of them really helped me, and gave me the courage to continue and believe that I can make a difference as a midwife. But than in itself can cause problems: cyber bullying, we have seen that. The more your profile is raised the more you expose yourself to scrutiny. I was seconded to Project Manager for Early Years agenda for Greater Manchester and the knives were out . I was devastated when my Head of Midwifery said that this was par for the course: try to better yourself and jealousy kicks in.
There are health and well-being initiatives in some trusts which need promoting. While we are there to do our work the public should remember we have children, elderly parents and our own problems like them, and sometimes we can’t leave it at the door as much as we try to, so compassion and understanding comes from both sides. I do not know of any midwife who comes to work to upset, harm or distress any woman or her family.”
So what do we need to do? What are you doing? What is happening in your Trust that is helping? Please share best practice and ideas – we are stronger when we work together.
Leigh Kendall opened this month for #MatExp with a call to action for Oxytocin October. The campaign is always action focused and we are keen to hear from anyone who is doing something to improve maternity experience in the UK, be it something big or something small. Yet we had already put together a number of blog posts with calls to action, back in #FlamingJune. So I decided that my action for this month would be to revisit those blog posts and find out what progress has been made.
The original blog posts were on these subjects (each subject links to the relevant post):
Having re-shared the posts on Facebook and Twitter I was delighted to see the responses coming in detailing what has changed, what has been started and what is continuing to be done. Take a look!
Perinatal Anxiety
Sarah McMullen of the NCT explained that she invited Emily Slater (MMHA Campaigns Manager) to speak and run a workshop at the NCT national conference – to raise awareness and inspire action. Sarah says that Emily’s plenary talk to 600+ staff, practitioners & volunteers “was incredibly powerful, and we’re meeting to discuss next steps for NCT”. Sarah added “We’ve also submitted two funding applications relating to mental health awareness (thanks to Rosey Wren for support), and have match-funded a PhD studentship with the wonderful Susan Ayres on Birth Trauma, and are supporting another PhD research project on group identity and PTSD”
Midwives on Twitter commented:
To read Jeannine and John’s blog post please click here. “You matter. I care.”
Emotional Wellbeing
#MatExp team member Emma Jane Sasaru has been incredibly active over the last few months. She has launched Unfold Your Wings a place of information and support aiming to raise awareness of Perinatal PTSD, birth trauma, reduce stigma and give sufferers hope. She has also launched a CoCreation Network community around perinatal mental health. Emma has then collaborated with #MatExp team member Susanne Remic to bring about a weekly #BirthTraumaChat on Twitter run jointly from Unfold Your Wings and Maternity Matters.
Also launched this month by West London Mental Health NHS Trust was this fantastic short film about perinatal mental health: https://vimeo.com/143359951 This film has already sparked many useful conversations.
In her talk at a recent National Maternity Review event, Baroness Julie Cumberlege made it very clear that the call for continuity of care is being heard by the review team up and down the country. Neighbourhood Midwives led a discussion at the review’s Birth Tank 2 event, and there were a couple of other discussions where options for continuity were also explored.
Midwife Deirdre Munro celebrated the launch of the new Global Village Midwives website this week. The movement is over a year old and Deirdre explains:
Infant Feeding
Lots of news about infant feeding from passionate individuals and voluntary organisations. On our #MatExp Facebook group Zoe Woodman explained: “In May we got approval from NCT to run a branch funded feeding support group. Started in June with an NCT bfc attending who is also an IBCLC. We are on 3 boundaries in terms of commissioning services so no local peer to peer style support groups were running within 8miles. The only service is an HV clinic once a week and it’s one on one so you have to wait outside the room to be seen. It’s been on our branch aims at our AMM since I’ve been chair (4yrs!) so finally chuffed to see it in action and I will get to use it myself in January for no3! It’s running twice a month currently but hope we can get funding in the future to run weekly. It’s slowly building in terms of attendance. Feedback so far is great!”
Claire Czjakowska’s Breastfeeding Advert is coming together and is looking very exciting – watch this space! Breastfeeding in Trafford launched its Twitter account this month so please follow for local breastfeeding news. BfN Portsmouth tweeted:
Midwifery students at the University of Worcester have launched a petition around the questionable practices of infant formula companies – follow the hashtag #WeakenTheFormula for more information.
As if this wasn’t enough, this month has seen the launch of the World Breastfeeding Trend Initiative for the UK. A committed group of individuals from the major breastfeeding voluntary organisations have come together to measure the country’s performance against the WHO Global Strategy for Infant and Young Child Feeding. Please visit the website for more information on how this project is structured and the indicators against which the UK will be measured. The project needs lots of input from families and professionals so please follow @wbtiuk on Twitter and find out how you can help.
Tongue Tie
Doula Zoe Walsh updated us: “We held a North West tongue-tie workshop in Blackpool. It’s now going on the MSLC agenda for Blackpool so that we can discuss local provision and see if it’s meeting the needs of local families.”
Breastfeeding and Medications
From a personal point of view, I finally got around to becoming a friend of the Drugs in Breastmilk Helpline this summer. The helpline is absolutely vital for ensuring that women get the correct information about what medications they can use when breastfeeding. The service is funded by the Breastfeeding Network and the charity once again asked supporters to do a #TeaBreakChallenge this month to help raise donations.
A wonderful #MatExp collaboration has sprung up this month between Angelique Fox, Sarah Baker and Wendy Jones. These two #MatExp mums who have never met in person have both volunteered to help Wendy to collect data and raise awareness with regards to drugs in breastmilk, particularly where dentists and podiatrists are concerned. It was discussed on the #MatExp Facebook group that these two healthcare professions are often cited as not having up to date information about breastfeeding and medications so this collaborative project is aiming to tackle that.
Luisa Lyons, the Infant Feeding Coordinator who wrote our original post on this subject, gave us this fantastic update: “Been a busy couple of months. Infant feeding e-learning training for doctors up and running at my unit and both paeds and obstetricians encouraged to complete it. Great support from our obstetric consultant clinicsdirector too. General paed nurses now doing mandatory infant feeding training every year. Been invited to teach general paed doctors face to face. Three GP’s have done the UNICEF 2 days bf management course with us and now writing bf training for GPs in Norfolk. Included info on bf and medications with scenarios to both student nurses and our midwives at keyworker training now, and incorporating into Mt for all maternity staff. Also off topic slightly am putting in a WHO code game to all the above which has generated lots of awareness with student midwives and maternity staff. Need to join DIBM as a friend which I had forgotten to do, so thanks for the heads up.”
Midwife Mark Harris launched his book this month, Men, Love and Birth, “the book about being present at birth that your lover wants you to read”.
A Manchester midwife reported positive outcomes around new rules enabling dads & partners to stay over on her unit:
When asked how we can best support Dads & Partners, newly elected NCT president Seana Talbot tweeted:
Community Outreach Midwife Wendy Warrington tweeted:
I asked Wendy about the work she does with regards to Dads & Partners and she explained “I talk about attachment and being with their baby, skin-to-skin touch. Antenatal and postnatal depression, and fathers’ role in supporting their partner in pregnancy, birth and beyond and how they can do this. I talk about baby cues and the impact of father’s involvement on child’s future emotional and cognitive development. I have had excellent feedback from parents and when I see them after the birth they say they felt well prepared for feeling and emotions experienced post birth. They love the fact that I talked about it”
Collaboration between Midwives and Health Visitors
Health visitors on the #MatExp Facebook group told us:
“My CPT & I have established 6 weekly meetings with the community midwife and the GP (whose special interest is pregnancy/neonates) to discuss cases”
“We already have that in my team we meet at least once a month with the midwife – it was weekly but we are very busy at the moment (both us and the midwife). She will just knock on our door though and share things – she really came on board with antenatal contacts telling parents to be and signposting those with small children with any worries to us.”
With excellent timing Sharon White, OBE, Professional Officer of the School & Public Health Nurses Association, then tweeted the updated pathway for health visiting and midwifery partnership.
And as a result of discussing all of this on Twitter, Sheena Byrom has invited me to lead a tweet chat with @WeMidwives and @WeHealthVisitor in November on the subject of midwife and health visitor collaboration. Watch this space!
And so much more has been happening in #OxyOct as well! #MatExp was well represented at the NHS Maternity Review’s Birth Tank 2 event in Birmingham – click here for Emma’s round up. I spoke at the launch of the Improving ME maternity review for Wirral, Merseyside, Warrington and West Lancashire – click here for my round up of the morning. Leigh Kendall and Florence Wilcock spread the word at the RCOG Conference on October 16th, and Leigh spoke at the Royal Society of Medicine event on October 20th.
Baby Loss Awareness Week took place this month and many important discussions were had around the subject of grief and loss, something which affects a number of #MatExp campaign members. Leigh wrote movingly about Standing on the Periphery for #HugosLegacy.
The RCM has this month launched its State of Maternity Services Report. Emma Jane Sasaru has written a series of three blogs about What Matters in Birth. Susanne Remic has been raising awareness of IUGR. Michelle Quashie created fantastic word clouds for display in her local maternity unit. We now have #MatExpHour every Friday created and launched by Louise Parry – click here for her round up of Week 2. So much going on!
I have no doubt there is much much more that I have missed from this round up. There is so much energy and passion in maternity services, and so much desire for change. Whatever it is you are trying to achieve, please join up with #MatExp via Twitter, Facebook or the website and get encouragement and input from like-minded people. Together we are stronger! Feel the Oxytocin flow!
As part of Oxytocin October (#OxyOct) I have been revisiting the first set of blog posts we put up calling for people to ACT in certain areas of maternity care. One of these was Time to Act for Dads & Partners, which included a mention of Mark Williams‘ work in this area.
Mark Williams is the founder of a new organisation called Dads Matter UK (Perinatal Mental Health for Fathers). He also founded Fathers Reaching Out, Youngness and Independent Mental Health Campaigners.
Father’s Reaching Out was set up in 2011 to raise awareness surrounding the detrimental impact that postnatal depression (PND) has on both fathers and equally families as a whole. Dads Matters UK aims to raise awareness of perinatal mental health, and educate every dad before the birth about birth trauma and PTSD for men.
We are delighted that Mark has written this blog post for #MatExp as part of #OxyOct.
______________________________________________
Depression can hit up to around one in five fathers by the time the child reaches adolescence. In a published report in 2015, it states that at least 10% of fathers will suffer with postnatal depression, which can include the birth itself and up to a year after. Fathers can develop lots of complications in this period, and this can influence their daily lives as well as affect their role within their family unit. It can impact heavily on their relationships, financial stability alongside lifestyle and emotional states. Emotional problems and psychological health needs are crucial elements to postnatal depression in fathers and need to be addressed. Fathers tend to get forgotten at this important and life changing event of having a baby, with mother and child being the centre of care delivery and rightly so, but we must remember there is a father there too. Fathers often get pushed aside which can result in feelings of isolation, anxiety and confusion at a time when they to need help.
Dads Matter UK is suggesting that the health service needs to develop a process for the screening and detecting of postnatal depression in fathers. As many fathers, the figures suggest, suffer with anxiety post birth of the child. The birth of a new baby can cause problems such as poor sleep, anxiety and stress. This can lead to problems within the relationship and fundamental communication processes within that relationship. After speaking to hundreds of fathers we are primarily concerned with the health of the father and their families. We feel that postnatal depression in fathers is equally significant and requires important consideration when implementing strategies and screening tools for postnatal depression. Fathers suffering with depression can feel increasingly pushed out and unsure of their role within the family thus affecting the bonding and attachment process between father and child.
Screening is important for men, as they are less likely to seek help and support. Particularly, in relation to their health problems. Due to the associated stigma towards mental health and its associated issues, young fathers are even more likely to be at risk and not seek the help they need. Men are often reluctant to admit that they may have an emotional problem or are unlikely to admit to feeling out of control. If this area of health is not addressed adequately this could lead to further breakdowns in the family structure and have long lasting devastating outcomes for our children.
We must remember that fathers can also suffer from PTSD at the birth. Post-traumatic Stress Disorder can occur following a life-threatening event like military combat, natural disasters, terrorist incidents, serious accidents, or violent personal assaults like rape. Most survivors of trauma return to normal given a little time. However, some people have stress reactions that don’t go away on their own, or may even get worse over time. These individuals may develop PTSD.
People who suffer from PTSD often suffer from nightmares, flashbacks, difficulty sleeping, and feeling emotionally numb. These symptoms can significantly impair a person’s daily life. As we know many suffer in silence and let post traumatic stress disorder effect all parts of their daily living. My own nightmares were what if my son had died and the thought of my wife being pregnant in the past did give me so much anxiety that at the time I didn’t know why.
PTSD is marked by clear physical and psychological symptoms. It often has symptoms like depression, substance abuse, problems of memory and cognition, and other physical and mental health problems. The disorder is also associated with difficulties in social or family life, including occupational instability, marital problems, family discord, and difficulties in parenting.
The “invisible wounds” of birth trauma-related PTSD affect not only the father or the family member, but also those around him or her. We must remember it effects everyone and education is needed to prepare the family for what may happen during and after the labour.
We run the risk of letting our fathers down at a time when we need to build strong families and communities for our future generations. Identifying the right support and providing improved health care in relation to Perinatal Mental Health is a top priority, so let’s ensure our health services have the right tools and services available to help and support fathers in relation to their partners’ postnatal depression. When screening fathers we must be mindful to remember that individuals are unique and have developed different styles of coping. It is important to respect the individual, involve them in their care and offer support to them as a person rather than just treat the illness.
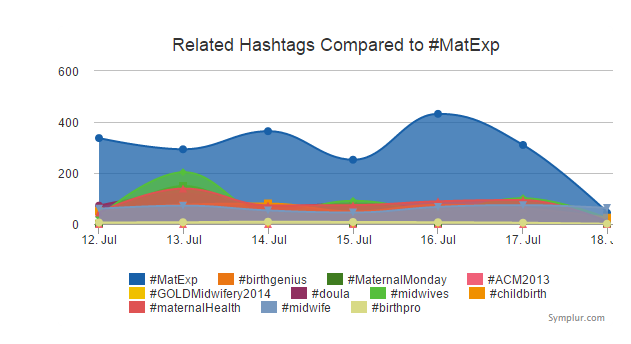
#MatExp has seen more interaction on social media than ones about similar issues (not that it’s a competition, but what is so brilliant about #MatExp is that there is no limit to the number or type of people who can get involved because it’s by everyone, for everyone).
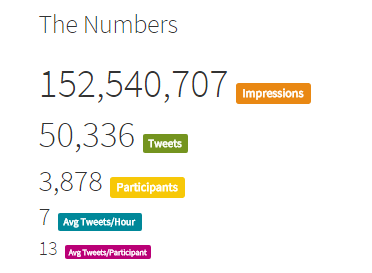
This next stat is VERY exciting:
Since #MatExp started being used as a hashtag there have been – drumroll please…
Yes you read that right – more than 152 million!
(Impressions means that Tweets bearing the #MatExp hashtag would have been seen on that number of timelines)
Guys and St Thomas’ Hospital held a Whose Shoes workshop, and seems to have inspired everyone who went, with 100% of attendees saying it would impact on their practise!
Being the language champion, I’ve been heartened to see so much chat about the issue with people from all sorts of professions and specialties taking on board the importance, value and impact of language.
Other language – such as ‘allow’ and ‘fail’ can have a devastating, enduring effect on a woman.
Culture can take a while to transform, of course, but the fact that we are able to have such conversations, and so openly too is a very positive start indeed.
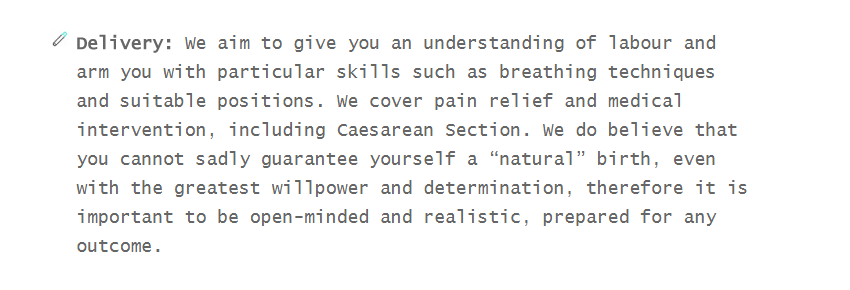
I was delighted to find this paragraph below on a site called lulubaby, which offers a range of courses to ‘prepare you for life with your baby’.
Words of common sense – “…you cannot sadly guarantee yourself a ‘natural birth’, even with the greatest willpower and determination…” fill my heart with joy. No mention of ‘low risk’ or ‘high risk’ either – let’s hope such common sense becomes much more common!
I am incredibly proud to have been named in the HSJ’s list of Patient Leaders, along with Ken Howard who designed our brilliant logo, and Alison Cameron, revolutionary extraordinaire.
Next week, I’m attending the listening event, the first of the National Maternity Review team’s activities. I’m going to be there as part of #HugosLegacy as well as #MatExp – I’ll be sharing my own experiences as well as thinking about how #MatExp can connect with the National Maternity Review team to make things happen. Flo and Gill are coming too – we spend so much time connecting on social media, it’s great to be able to catch up face-to-face sometimes too.
So! We’ve been rather busy. Which is why we have been seeking ways to create more hours in the day, such as getting a job lot of time-turners, like Harry Potter’s Hermione.
And we’re going to need them, because after the summer we have LOADS of exciting things going on, such as NHS Expo, and a #MatExp conference – watch this space! I’m looking forward to meeting even more of the #MatExp community, many of whom have become friends at these events.
All of the #MatExp community are busy doing something positive every day, of course. A huge THANK YOU to you all. These are for you for taking the time to get involved, share your stories and to make a difference to women, babies and their families. Forget-me-nots are very special flowers!
There is so much going on – Helen, Emma, and Susanne are also capturing as much as they can in their fab posts; it’s impossible to capture everything, but please know that every action and activity, whether big or small is greatly appreciated.
A couple of final thoughts…
You don’t need to ask for permission (besides the obvious!) – JFDI!and always remember…
There have been some fantastic conversations taking place on the MatExp Facebook group, with lots of ACTION threads being posted to generate discussion. The aim of these discussions is to identify ways that we can ACT to improve maternity experiences. Big, long-term actions that might require system change or a change in culture. And small, immediate actions, that professionals and individuals can take today to improve the maternity experience of those around them.
Over the last six months two big themes have emerged from #MatExp for me. The first is WHY are so many age-old issues still a problem for maternity care in this country? The answer to me is the working environment midwives face, as discussed here. The second is HOW can we make a real difference to family’s maternity experiences? So many actions have come out of #MatExp but the one that stands head and shoulders above, in my opinion, is continuity of care.
I don’t mean Ed Milliband’s diluted version of “the same midwife throughout labour”. I mean the same midwife antenatally, during labour and postnatally, or the same team of two or three midwives for the whole of that period. Women who hire independent midwives or who have access to OnetoOne Midwives have this type of continuity antenatally and postnatally, but they only have those same midwives during labour if they give birth at home. IMs and OnetoOne are not insured to act as midwives in hospital settings, although they can accompany women to hospital as advocates. Doulas are also with women as advocates and support for the whole of their pregnancy, birth and postnatal period but they are not qualified to act as midwives.
When I brought up continuity of care as an ACTION thread on Facebook, I asked the following questions:
What are the barriers to providing continuity of care on the NHS? Is it as simple as not enough midwives, or is there more to it than that?
As an anxious person I really prioritised continuity of care, so used an independent midwife in my first pregnancy and a OnetoOne midwife in my second. What would my options have been on the NHS, under what circumstances can women be put onto a one-to-one care pathway?
What ACTION can we take to make continuity of care a reality?
What ACTION can we take to build good relationships between women and their midwifery teams where continuity of care is NOT a reality?
The suggested actions from the discussion that followed were:
Demonstrate the benefits of caseloading to NHS midwives
Strong leaders at the helm of trusts who themselves understand how to implement and lead their midwives into wanting continuity of care
NHS trusts to talk to independent midwives and social enterprise midwives who are the knowledgeable ones when it comes to providing continuity
Think about options for a team approach. One group member directed us to look at the Streatham Valley midwife team: “They were part of a pilot scheme for community midwives where you saw the same midwife and often they came to you for booking in and later appointments. They also checked you at home when in labour to avoid wasted trips to hospital and they have an excellent home birth record. Out of my ante natal group of 5 first time mum’s none of us had anything stronger than gas and air we had one home birth and only one use of forceps. They are amazing.”
Understand the positive impact that continuity of carer can have on patient safety and infant mortality
Find ways to care for midwives and avoid the “burn out” that is often associated with a caseloading model of working
Women with more complex pregnancies to be caseloaded by a team expert in their complexities – in other words, being at a higher risk of complications should not exclude women from continuity of care, in fact if anything these women need it more
Consider personalised budgets ( i.e. the NHS would allocate a woman funding to choose the service they wish) and whether or not this concept could help in delivering continuity of care
If continuity is not available then note-keeping needs to be excellent so women don’t always have to repeat themselves (which can be particularly hard following baby loss), and so that plans can be discussed and followed up
Women who are vulnerable or at risk of perinatal mental health problems should be at the front of the queue for continuity of care
Ensure that families are aware of and understand any choices they do have when it comes to their maternity care team
One healthcare professional commented “The commonest refrain you hear from mothers these days is ‘I never saw the same midwife twice’; this is a great sadness to me as surely the greatest gift to mediate the stressful vocation that is midwifery, is the relationship you develop with your ladies.”
Another woman who had opted for independent midwifery care in her second pregnancy commented “I just needed to know that someone was going to know me personally and take my wishes/needs seriously.”
Continuity of care was the strongest theme in the feedback to the National Maternity Review provided by my private Facebook group. It comes up time and again in discussions – I was discussing it today with student midwives at Salford University and they agreed that many midwives want to work to a caseloading model as much as families do. It just has to be constructed in a way that makes it feasible for midwives, many of whom have young families themselves.
Campaign for Choice
This is not news. The RCM’s Better Births campaign has continuity of care as one of its key themes. The demand for caseloading from families accounts for the popularity of OnetoOne midwives in the areas where they are commissioned. A group of mothers in Greater Manchester is campaigning for the local CCGs to make this service available to women, and as someone who has benefited from that company’s care I joined them on a demonstration in Manchester city centre. If continuity is not going to be available on the NHS then OnetoOne might be the best option for families, although as this post of mine shows not all women find that the various services work together.
What I find striking is how much continuity of care would impact on other areas where the #MatExp campaign has asked for ACTION. Anxiety is reduced if women know their carers. Emotional well-being is improved as are infant feeding outcomes. Dads & partners have more chance of being involved and having their own struggles recognised if they are able to get to know the family’s care team. It will be far easier for midwives and health visitors to collaborate if it is clear who is looking after which families.
I was delighted when an insurance solution was found for independent midwifery in this country. I also have high praise for the model of care provided by OnetoOne. Support and advocacy from a doula can be invaluable. But continuity of care should not be on the periphery of the UK maternity experience. It should BE the UK maternity experience.